

Temporal trends in treatment of ST-elevation myocardial infarction among men and women in Switzerland between 1997 and 2011
- PMID: 24062906
- PMCID: PMC3760536
- DOI: 10.1177/2048872612454021
Temporal trends in treatment of ST-elevation myocardial infarction among men and women in Switzerland between 1997 and 2011
Abstract
Background: Few data are available concerning the impact of gender on temporal trends in patients with acute ST-segment elevation myocardial infarction (STEMI).
Methods: All STEMI patients consecutively enrolled in the AMIS (Acute Myocardial Infarction in Switzerland) Plus project from 1997-2011 were included. Temporal trends in presentation, treatment and outcomes were analyzed using multiple logistic regressions with generalized estimations.
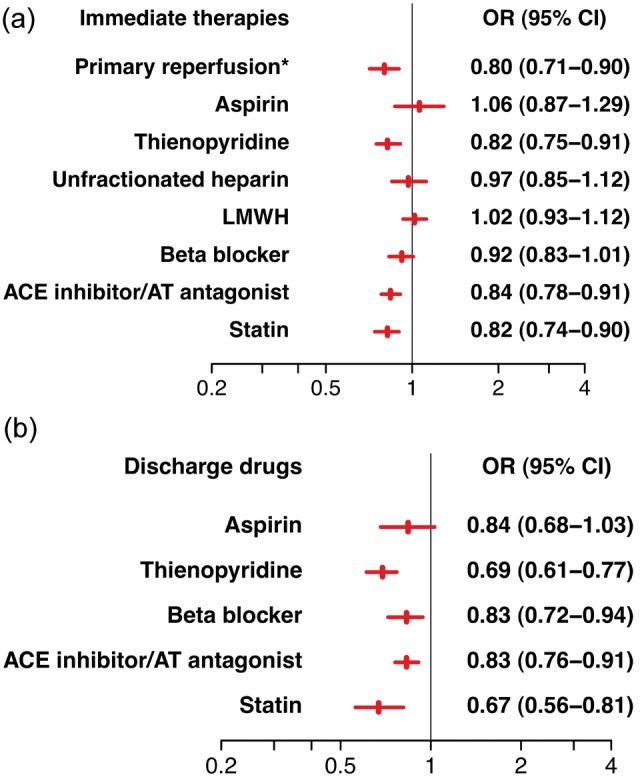
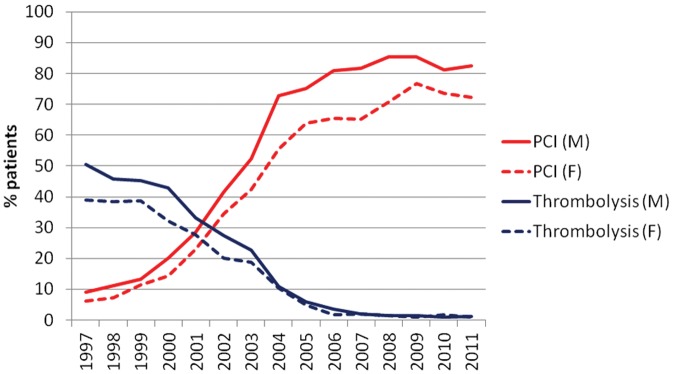
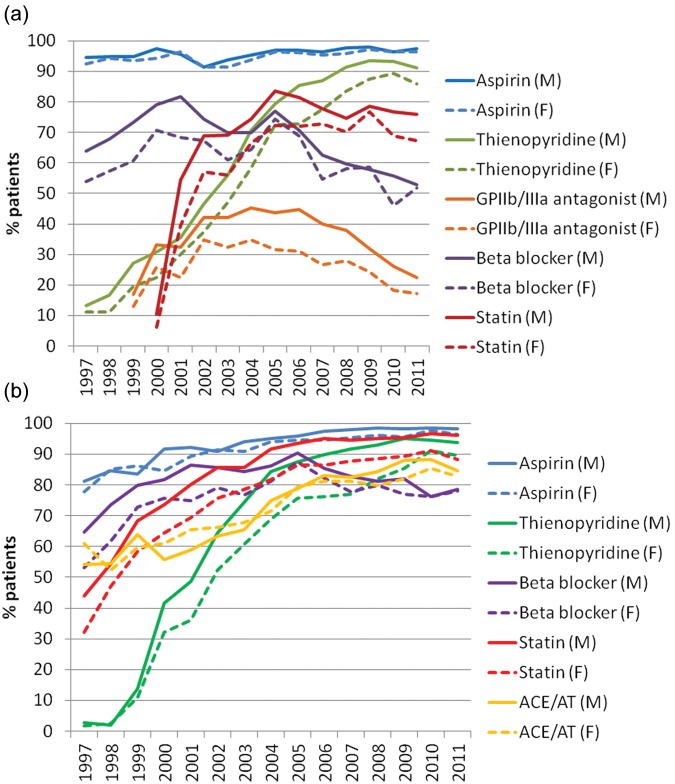
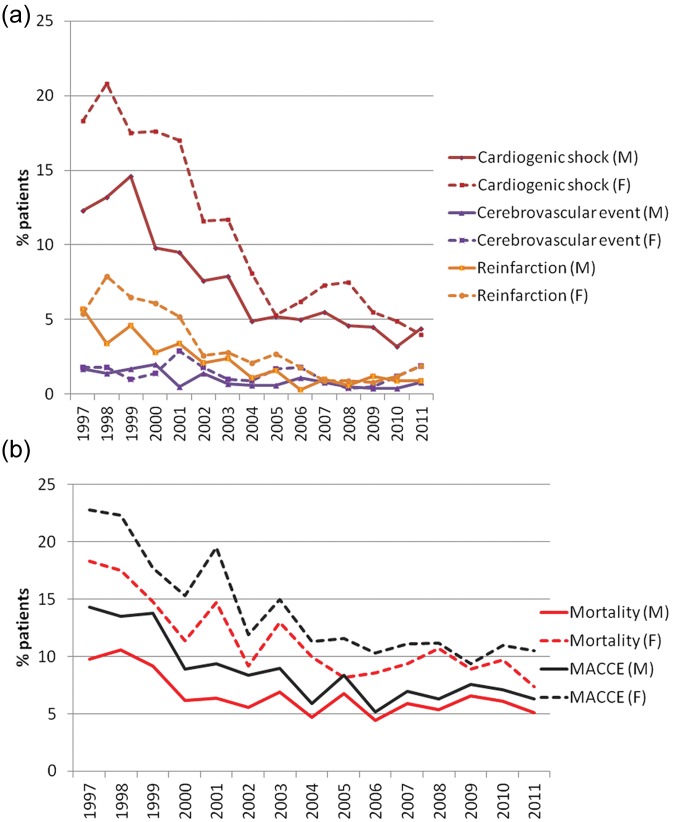
Results: Of 21,620 STEMI patients, 5786 were women and 15,834 men from 78 Swiss hospitals. Women were 8.6 years older, presented 48 minutes later with less pain, but more dyspnea, and more frequently had atrial fibrillation (5.5 vs. 3.9%, p<0.001), heart failure (Killip class >2) (9.7 vs. 7.3%, p<0.001), and moderate or severe comorbidities (24.8 vs. 18.2%, p<0.001). Women were less likely to undergo primary reperfusion treatment after adjustment for baseline characteristics and admission year (OR 0.80, 95% CI 0.71-0.90, p<0.001) or receive early and discharge drugs, such as thienopyridines, angiotensin-converting-enzyme inhibitors, angiotensin II receptor antagonists, and statins. In 1997, thrombolysis was performed in 51% of male and 39% of female patients; its use rapidly decreased during the 1990s and has now become negligible. Primary percutaneous coronary intervention increased from under 10% in both genders in 1997 to over 70% in females and over 80% in males since 2006. Patients admitted in cardiogenic shock increased by 8% per year in both genders. The incidence of both reinfarction and cardiogenic shock developing during hospitalization decreased significantly over 15 years while in-hospital mortality decreased from 10 to 5% in men and from 18 to 7% in women. This corresponds to a relative reduction of 5% per year for males (OR 0.95, 95% CI 0.92-0.99, p=0.006) and 6% per year for female STEMI patients (OR 0.94, 95% CI 0.91-0.97, p<0.001). Despite higher crude in-hospital mortality, female gender per se was not an independent predictor of in-hospital mortality (OR 1.07, 95% CI 0.84-1.35, p=0.59).
Conclusion: Substantial changes have occurred in presentation, treatment, and outcome of men and women with STEMI in Switzerland over the past 15 years. Although parallel trends were seen in both groups, ongoing disparities in certain treatments remain. However, these did not translate into worse risk-adjusted in-hospital mortality, suggesting that the gender gap in STEMI care may be closing.
Keywords: Acute myocardial infarction; evidence-based medicine; primary angioplasty; sex; trends.
Conflict of interest statement
Figures
References
-
- Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group. Lancet 1994; 343: 311–322 - PubMed
-
- Bates ER, Nallamothu BK. Commentary: the role of percutaneous coronary intervention in ST-segment-elevation myocardial infarction. Circulation 2008; 118: 567–573 - PubMed
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003; 361: 13–20 - PubMed
-
- Antman EM, Hand M, Armstrong PW, et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction, writing on behalf of the 2004 Writing Committee. Circulation 2008; 117: 296–329 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
