

An assessment of composite measures of hospital performance and associated mortality for patients with acute myocardial infarction. Analysis of individual hospital performance and outcome for the National Institute for Cardiovascular Outcomes Research (NICOR)
- PMID: 24062929
- PMCID: PMC3760578
- DOI: 10.1177/2048872612469132
An assessment of composite measures of hospital performance and associated mortality for patients with acute myocardial infarction. Analysis of individual hospital performance and outcome for the National Institute for Cardiovascular Outcomes Research (NICOR)
Abstract
Aim: To investigate whether a hospital-specific opportunity-based composite score (OBCS) was associated with mortality in 136,392 patients with acute myocardial infarction (AMI) using data from the Myocardial Ischaemia National Audit Project (MINAP) 2008-2009.
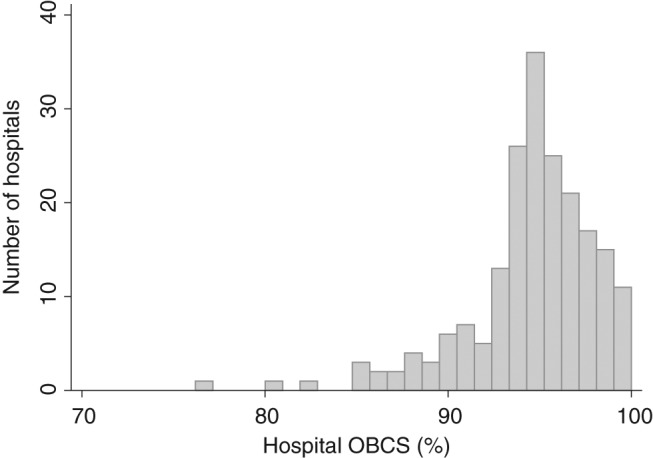
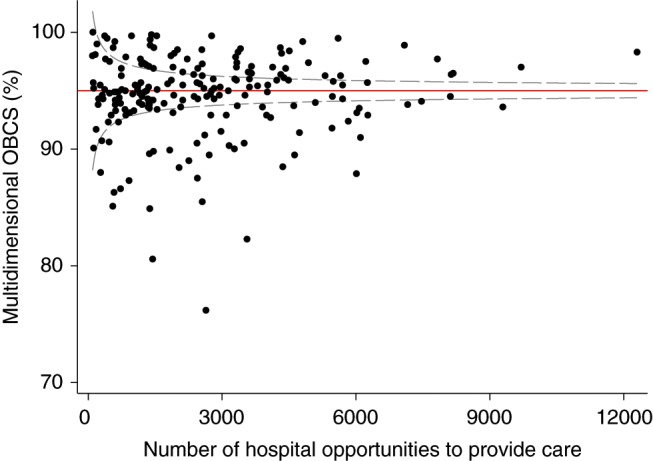
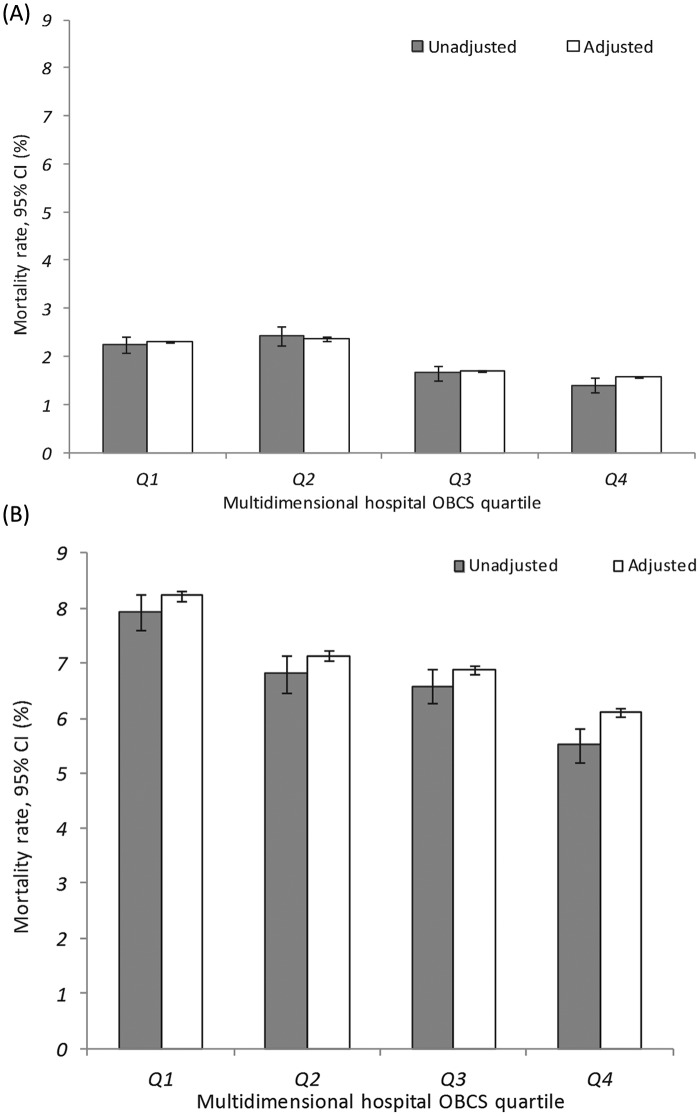
Methods and results: For 199 hospitals a multidimensional hospital OBCS was calculated on the number of times that aspirin, thienopyridine, angiotensin-converting enzyme inhibitor (ACEi), statin, β-blocker, and referral for cardiac rehabilitation was given to individual patients, divided by the overall number of opportunities that hospitals had to give that care. OBCS and its six components were compared using funnel plots. Associations between OBCS performance and 30-day and 6-month all-cause mortality were quantified using mixed-effects regression analysis. Median hospital OBCS was 95.3% (range 75.8-100%). By OBCS, 24.1% of hospitals were below funnel plot 99.8% CI, compared to aspirin (11.1%), thienopyridine (15.1%), β-blockers (14.7%), ACEi (19.1%), statins (12.1%), and cardiac rehabilitation (17.6%) on discharge. Mortality (95% CI) decreased with increasing hospital OBCS quartile at 30 days [Q1, 2.25% (2.07-2.43%) vs. Q4, 1.40% (1.25-1.56%)] and 6 months [Q1, 7.93% (7.61-8.25%) vs. Q4, 5.53% (5.22-5.83%)]. Hospital OBCS quartile was inversely associated with adjusted 30-day and 6-month mortality [OR (95% CI), 0.87 (0.80-0.94) and 0.92 (0.88-0.96), respectively] and persisted after adjustment for coronary artery catheterization [0.89 (0.82-0.96) and 0.95 (0.91-0.98), respectively].
Conclusions: Multidimensional hospital OBCS in AMI survivors are high, discriminate hospital performance more readily than single performance indicators, and significantly inversely predict early and longer-term mortality.
Keywords: Acute myocardial infarction; composite performance indicators; mortality; performance; quality of care.
Conflict of interest statement
Figures

References
-
- Gale CP, Cattle BA, Woolston A, et al. Resolving inequalities in care? Reduced mortality in the elderly after acute coronary syndromes. The Myocardial Ischaemia National Audit Project 2003–2010. Eur Heart J 2012; 33: 630–639 - PubMed
-
- Fox KA, Goodman SG, Klein W, et al. Management of acute coronary syndromes. Variations in practice and outcome; findings from the Global Registry of Acute Coronary Events (GRACE). Eur Heart J 2002; 23: 1177–1189 - PubMed
-
- Fonarow GC, Albert NM, Curtis AB, et al. Associations between outpatient heart failure process-of-care measures and mortality/clinical perspective. Circulation 2011; 123: 1601–1610 - PubMed
