

Strategic target temperature management in myocardial infarction--a feasibility trial
- PMID: 24064228
- PMCID: PMC3812852
- DOI: 10.1136/heartjnl-2013-304624
Strategic target temperature management in myocardial infarction--a feasibility trial
Abstract
Objective: The purpose of this study was to demonstrate the feasibility of a combined cooling strategy started out of hospital as an adjunctive to percutaneous coronary intervention (PCI) in the treatment of ST-elevation acute coronary syndrome (STE-ACS).
Design: Non-randomised, single-centre feasibility trial.
Setting: Department of emergency medicine of a tertiary-care facility, Medical University of Vienna, Vienna, Austria. In cooperation with the Municipal ambulance service of the city of Vienna.
Patients: Consecutive patients with STE-ACS presenting to the emergency medical service within 6 h after symptom onset.
Interventions: Cooling was initiated with surface cooling pads in the out-of-hospital setting, followed by the administration of 1000-2000 mL of cold saline at hospital arrival and completed by endovascular cooling in the catheterisation laboratory.
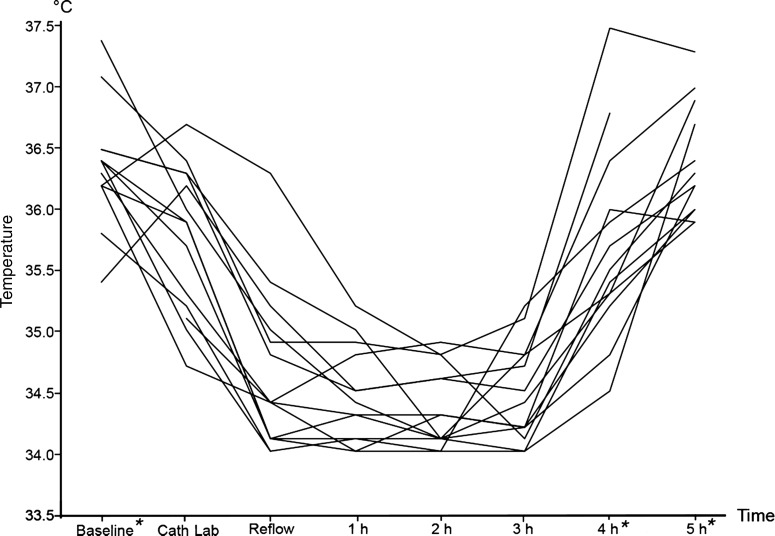
Main outcome measures: Feasibility of lowering core temperature below 35.0°C prior to immediately performed revascularisation. Safety and tolerability of the cooling procedure.
Results: In enrolled 19 patients (one woman, median age 51 years (IQR 45-59)), symptom onset to first medical contact (FMC) was 45 min (IQR 31-85). A core temperature below 35.0°C at reperfusion of the culprit lesion was achieved in 11 patients (78%) within 100 min (IQR 90-111) after FMC without any cooling-related serious adverse event. Temperature could be lowered from baseline 36.4°C (IQR 36.2-36.5°C) to 34.4°C (IQR 34.1-35.0°C) at the time of reperfusion.
Conclusions: With limitations an immediate out-of-hospital therapeutic hypothermia strategy was feasible and safe in patients with STE-ACS undergoing primary PCI.
Clinical trial registration: http://www.clinicaltrials.gov/ct2/show/NCT01864343; clinical trials unique identifier: NCT01864343.
Keywords: Coronary Artery Disease; Myocardial Ischaemia and Infarction (IHD).
Figures
References
-
- Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC) Steg PG, James SK, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2012;33:2569–619 - PubMed
-
- Yellon DM, Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med 2007;357:1121–35 - PubMed
-
- Miller TD, Christian TF, Hopfenspirger MR, et al. Infarct size after acute myocardial infarction measured by quantitative tomographic 99mTc sestamibi imaging predicts subsequent mortality. Circulation 1995;92:334–41 - PubMed
-
- Burns RJ, Gibbons RJ, Yi Q, et al. The relationships of left ventricular ejection fraction, end-systolic volume index and infarct size to six-month mortality after hospital discharge following myocardial infarction treated by thrombolysis. J Am Coll Cardiol 2002;39:30–6 - PubMed
-
- Hypothermia after Cardiac Arrest Study Group Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346:549–56 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous