

Morbidity risks among older adults with pre-existing age-related diseases
- PMID: 24064264
- PMCID: PMC3895485
- DOI: 10.1016/j.exger.2013.09.005
Morbidity risks among older adults with pre-existing age-related diseases
Abstract
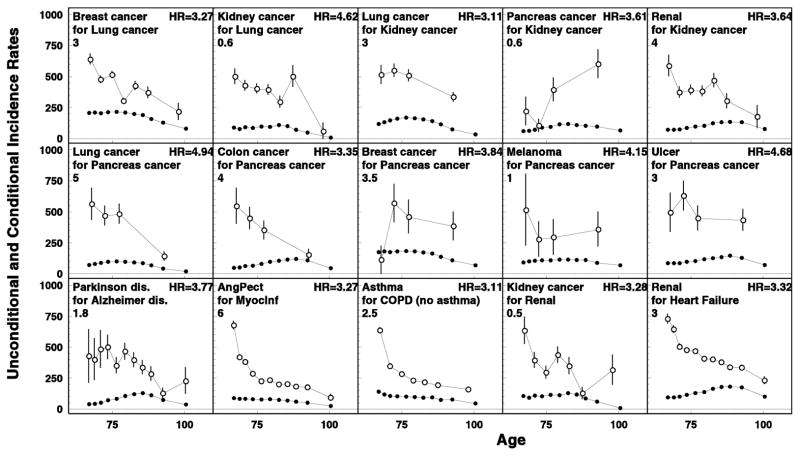
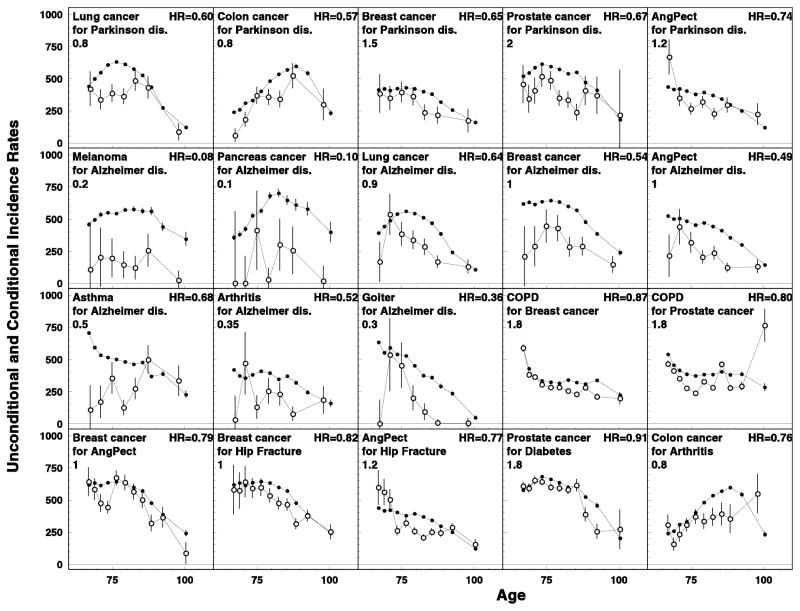
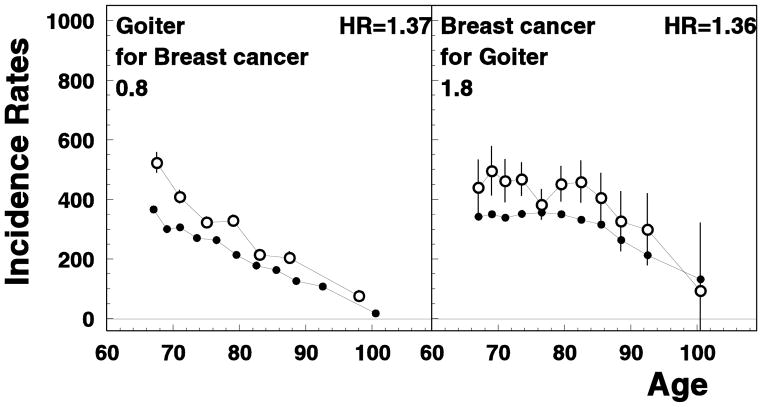
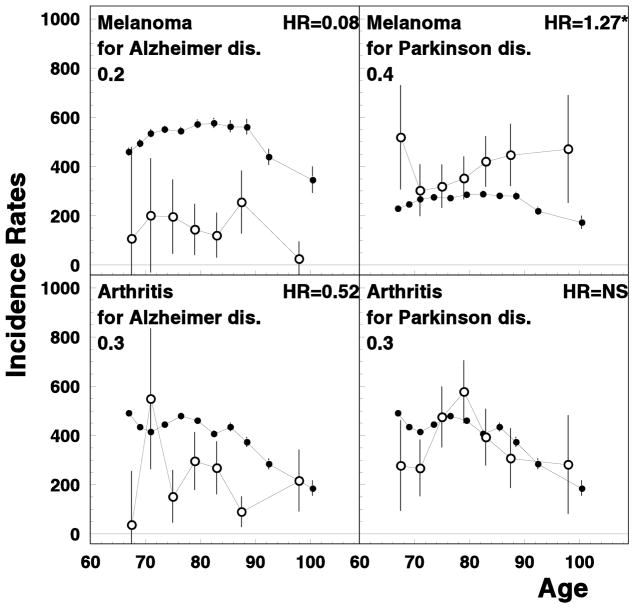
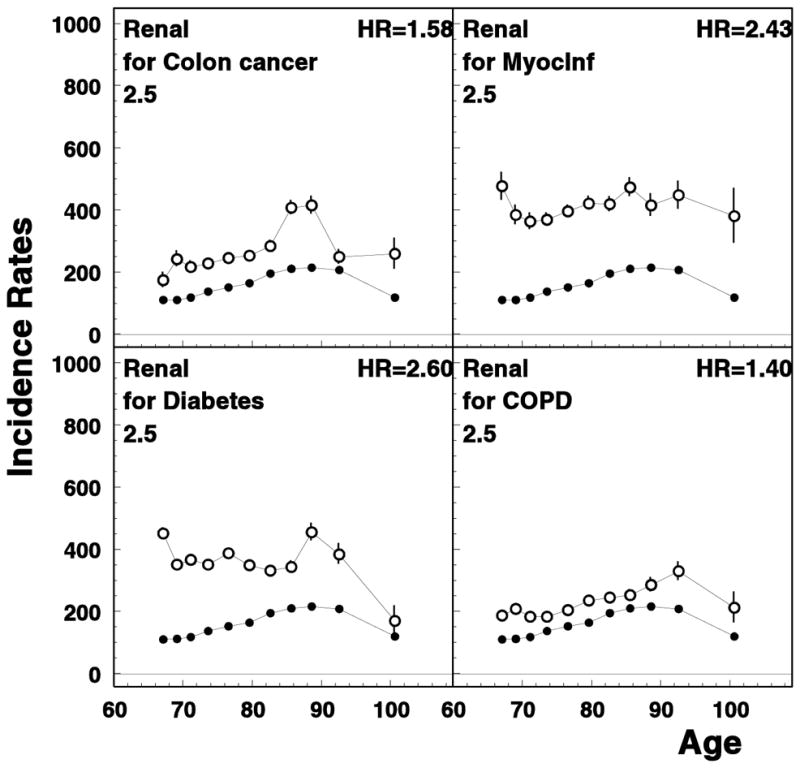
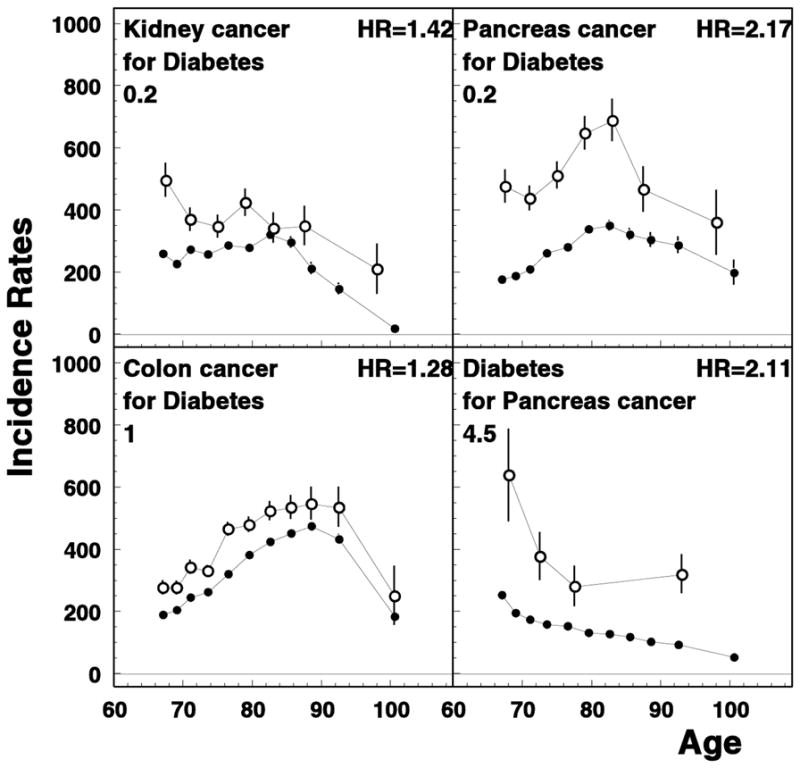
Multi-morbidity is common among older adults; however, for many aging-related diseases there is no information for U.S. elderly population on how earlier-manifested disease affects the risk of another disease manifested later during patient's lifetime. Quantitative evaluation of risks of cancer and non-cancer diseases for older adults with pre-existing conditions is performed using the Surveillance, Epidemiology, and End Results (SEER) Registry data linked to the Medicare Files of Service Use (MFSU). Using the SEER-Medicare data containing individual records for 2,154,598 individuals, we empirically evaluated age patterns of incidence of age-associated diseases diagnosed after the onset of earlier manifested disease and compared these patterns with those in general population. Individual medical histories were reconstructed using information on diagnoses coded in MFSU, dates of medical services/procedures, and Medicare enrollment/disenrollment. More than threefold increase of subsequent diseases risk was observed for 15 disease pairs, majority of them were i) diseases of the same organ and/or system (e.g., Parkinson disease for patients with Alzheimer disease, HR=3.77, kidney cancer for patients with renal failure, HR=3.28) or ii) disease pairs with primary diseases being fast-progressive cancers (i.e., lung, kidney, and pancreas), e.g., ulcer (HR=4.68) and melanoma (HR=4.15) for patients with pancreatic cancer. Lower risk of subsequent disease was registered for 20 disease pairs, mostly among patients with Alzheimer's or Parkinson's disease, e.g., decreased lung cancer risk among patients with Alzheimer's (HR=0.64) and Parkinson's (HR=0.60) disease. Synergistic and antagonistic dependences in geriatric disease risks were observed among US elderly confirming known and detecting new associations of wide spectrum of age-associated diseases. The results can be used in optimization of screening, prevention and treatment strategies of chronic diseases among U.S. elderly population.
Keywords: Aging; Chronic disease onset; Comorbidity; Dependent risks; Geriatric disease; Medicare.
© 2013.
Figures
References
-
- Anderson G Solutions JHUPf & Foundation RWJ. Chronic conditions: Making the case for ongoing care. Johns Hopkins University; 2004.
-
- Boffetta P, Ye W, Boman G, Nyren O. Lung cancer risk in a population-based cohort of patients hospitalized for asthma in Sweden. European Respiratory Journal. 2002;19(1):127–133. - PubMed
-
- Cann SA, van Netten JP, van Netten C. Hypothesis: iodine, selenium and the development of breast cancer. Cancer Causes and Control. 2000;11(2):121–127. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
