

The effect of steep Trendelenburg positioning on intraocular pressure and visual function during robotic-assisted radical prostatectomy
- PMID: 24064941
- PMCID: PMC3933168
- DOI: 10.1136/bjophthalmol-2013-303536
The effect of steep Trendelenburg positioning on intraocular pressure and visual function during robotic-assisted radical prostatectomy
Abstract
Background: To evaluate intraocular pressure (IOP) changes in patients undergoing robotic-assisted radical prostatectomy and to evaluate complications from increased IOP.
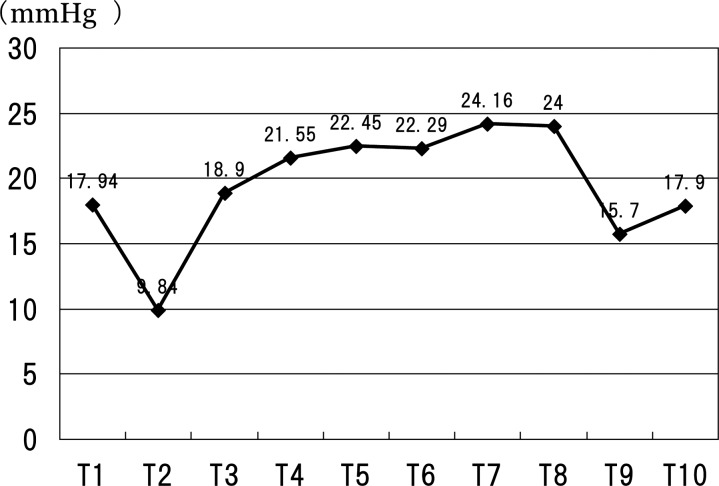
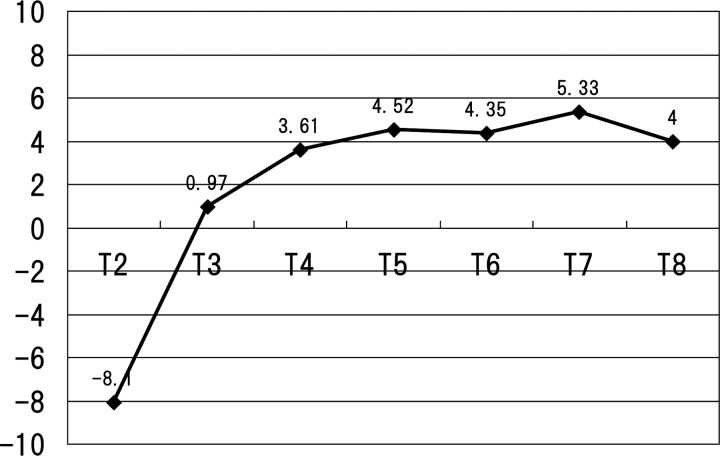
Methods: Thirty-one eyes scheduled for robotic prostatectomy were included. Perioperative IOP measurements were performed as follows: prior to induction of anaesthesia while supine and awake (T1); immediately post-induction while supine (T2); every hour from 0 to 5 h while anaesthetised in a steep Trendelenburg position (T3-T8); prior to awakening while supine (T9); and 30 min after awakening while supine (T10). A complete ophthalmic examination including visual acuity and retinal nerve fibre layer thickness (RNFL) was performed at enrolment and 1 month postoperatively.
Results: Average IOP (mm Hg) for each time point was as follows: T1=18.0, T2=9.8, T3=18.9, T4=21.6, T5=22.5, T6=22.3, T7=24.2, T8=24.0, T9=15.7 and T10=17.9. The proportion of eyes with intraoperative IOP ≧30 mm Hg were as follows: T3=0%, T4=3.23%, T5=9.68%, T6=6.45%, T7=22.22%, and T8=25%. Maximum IOP was 36 mm Hg. Mean visual acuity (logarithm of the minimal angle of resolution) and RNFL showed no statistically significant difference before and after operation and no other ocular complications were found at final examination.
Conclusions: While IOP increased in a time-dependent fashion in anesthaetised patients undergoing robotic-assisted radical prostatectomy in a steep Trendelenburg position, visual function showed no significant change postoperatively and no complications were seen. Steep Trendelenburg positioning during time-limited procedures appears to pose little or no risk from IOP increases in patients without pre-existing ocular disease.
Keywords: Glaucoma; Intraocular Pressure.
Figures
References
-
- Weber ED, Colyer MH, Lesser RL, et al. Posterior ischemic optic neuropathy after minimally invasive prostatectomy. J Neuroophthalmol 2007;27:285–7 - PubMed
-
- Awad H, Santilli S, Ohr M, et al. The effects of steep Trendelenburg positioning on intraocular pressure during robotic radical prostatectomy. Anesth Analg 2009;109:473–8 - PubMed
-
- Donlon JV, Jr, Doyle DJ, Feld man MA. Anethesia for eye, ear, nose and throat surgery. In Miller RD, ed. Miller's anesthesia. 6th edn Philadelphia: Elsevier, Churchill Livingstone, 2005
-
- Grunwald JE, Pitz J, Hariprasad SM, et al. Optic nerve and choroidal circulation in glaucoma. Invest Ophthalmol Vis Sci 1998;39:2329–36 - PubMed
-
- Buskirk EMV, Cioffi GA. Glaucomatous optic neuropathy. Am J Ophthalmol 1992;113:447–52 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials