

Recurrent urinary tract infections among women: comparative effectiveness of 5 prevention and management strategies using a Markov chain Monte Carlo model
- PMID: 24065333
- PMCID: PMC3871790
- DOI: 10.1093/cid/cit646
Recurrent urinary tract infections among women: comparative effectiveness of 5 prevention and management strategies using a Markov chain Monte Carlo model
Abstract
Background: Recurrent urinary tract infections (UTIs) are a common problem among women. However, comparative effectiveness strategies for managing recurrent UTIs are lacking.
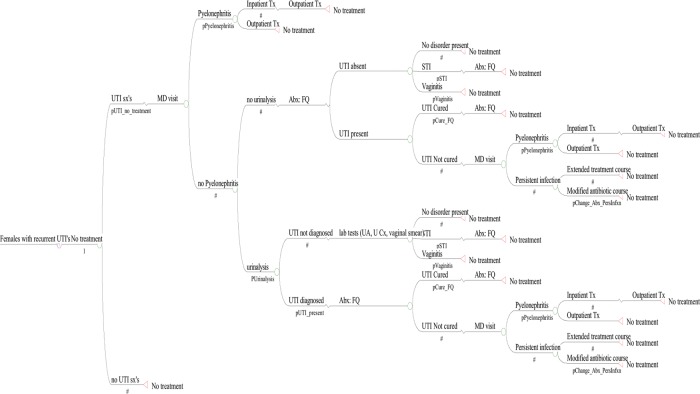
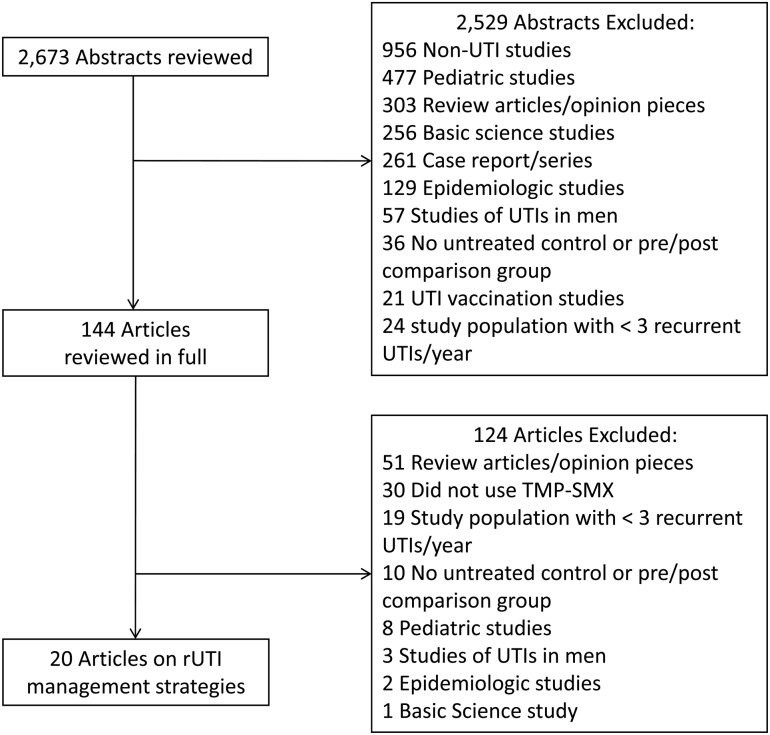
Methods: We performed a systematic literature review of management of women experiencing ≥3 UTIs per year. We then developed a Markov chain Monte Carlo model of recurrent UTI for each management strategy with ≥2 adequate trials published. We simulated a cohort that experienced 3 UTIs/year and a secondary cohort that experienced 8 UTIs/year. Model outcomes were treatment efficacy, patient and payer cost, and health-related quality of life.
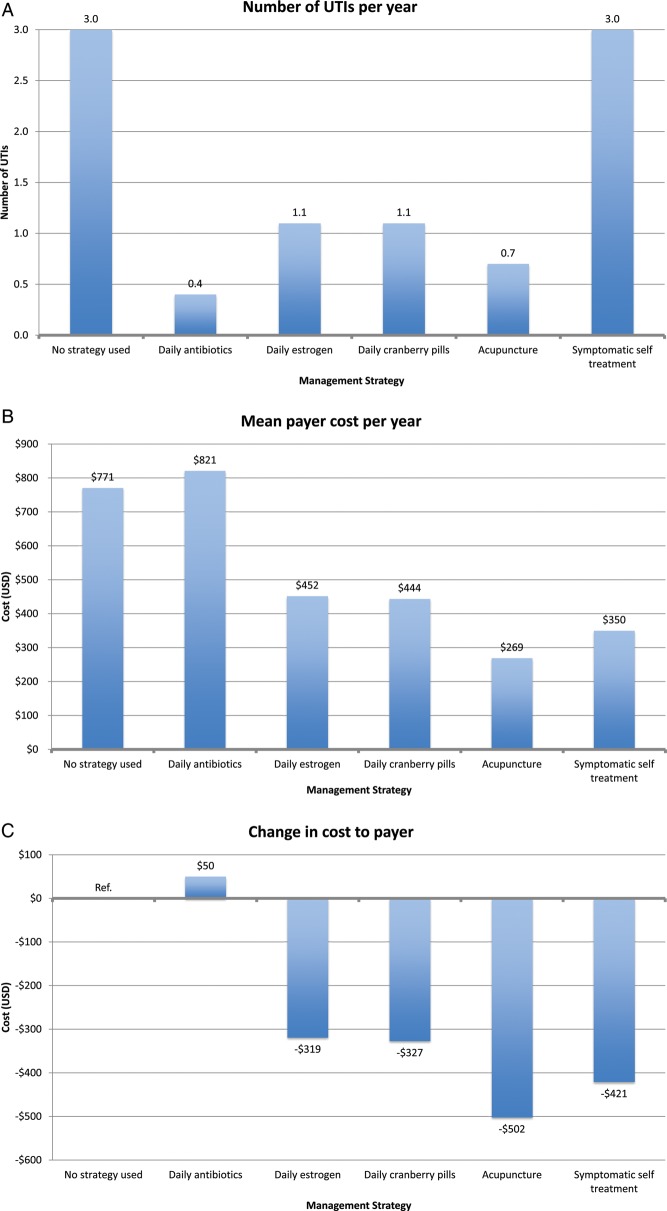
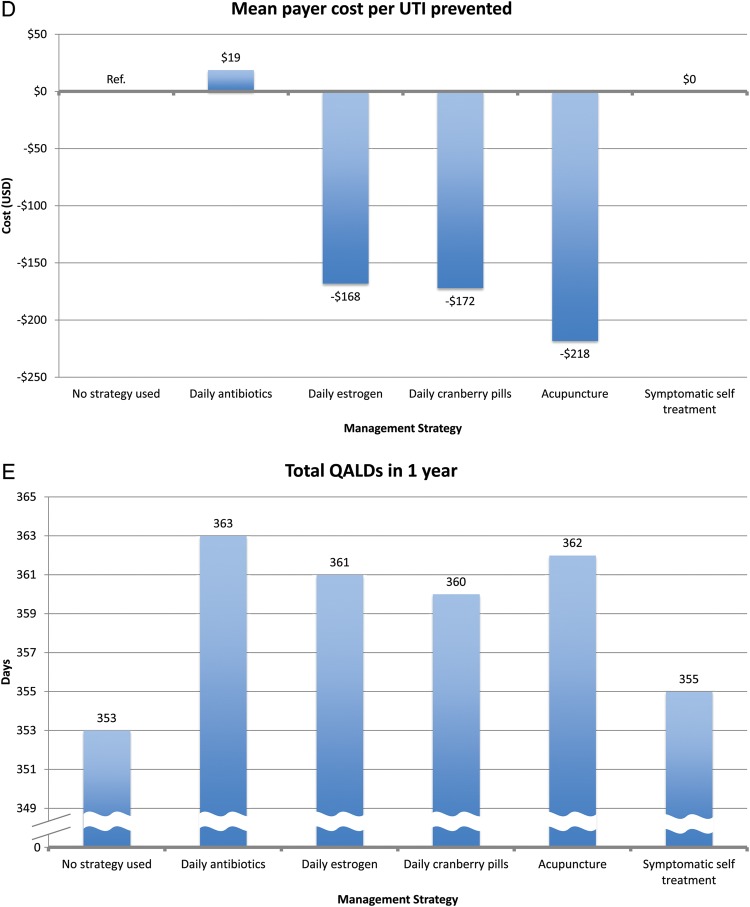
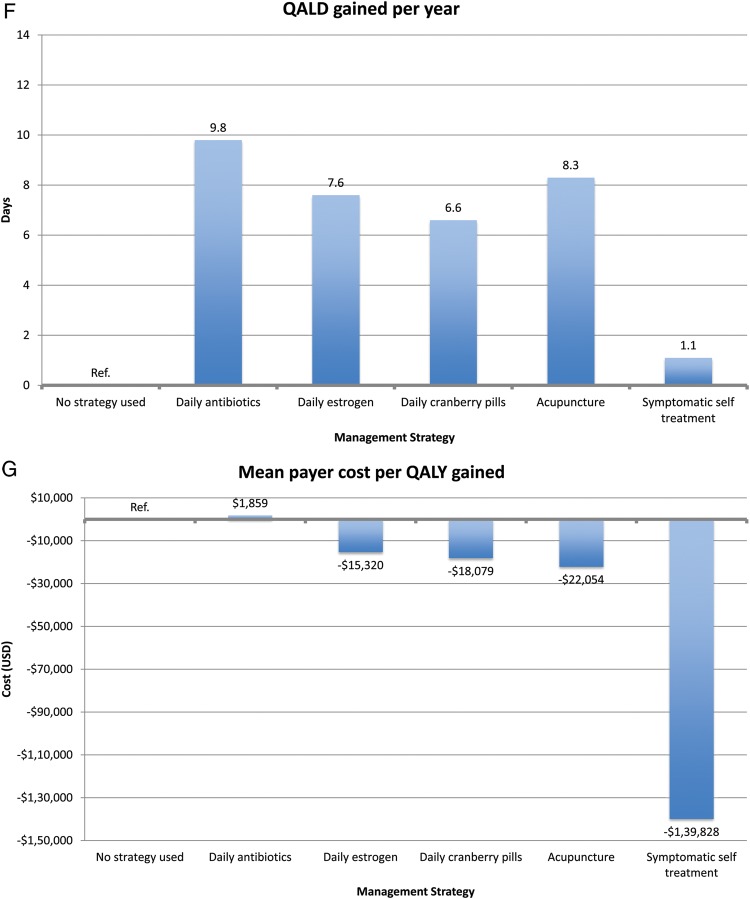
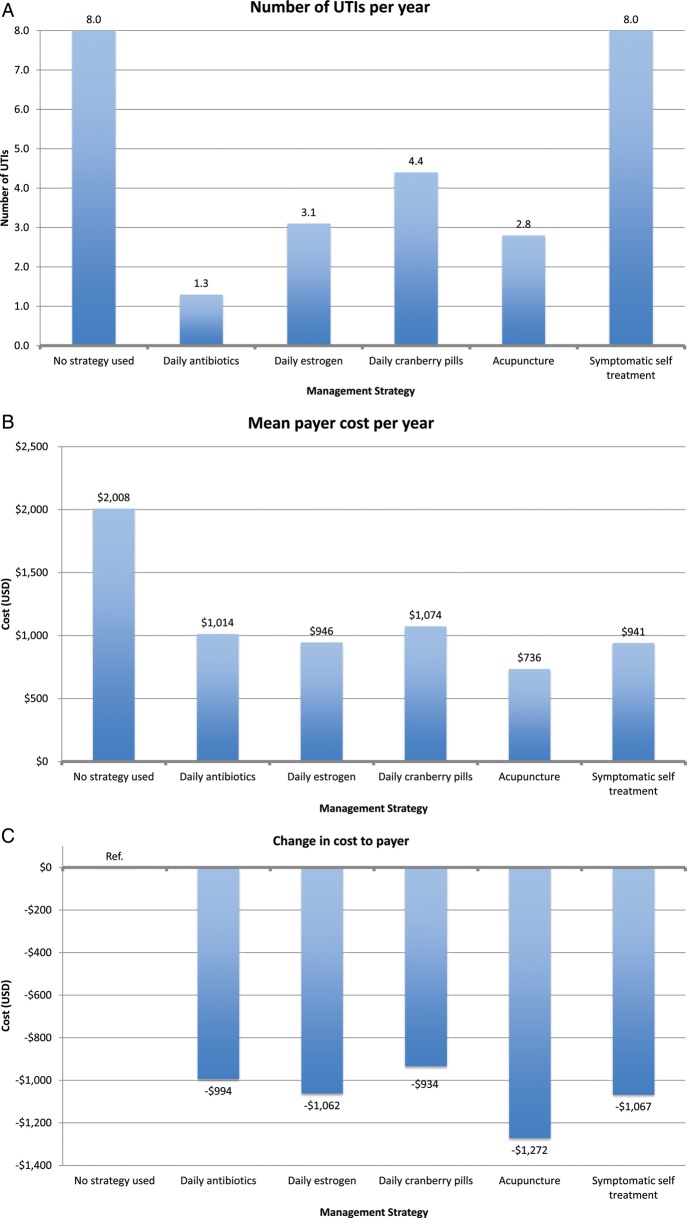
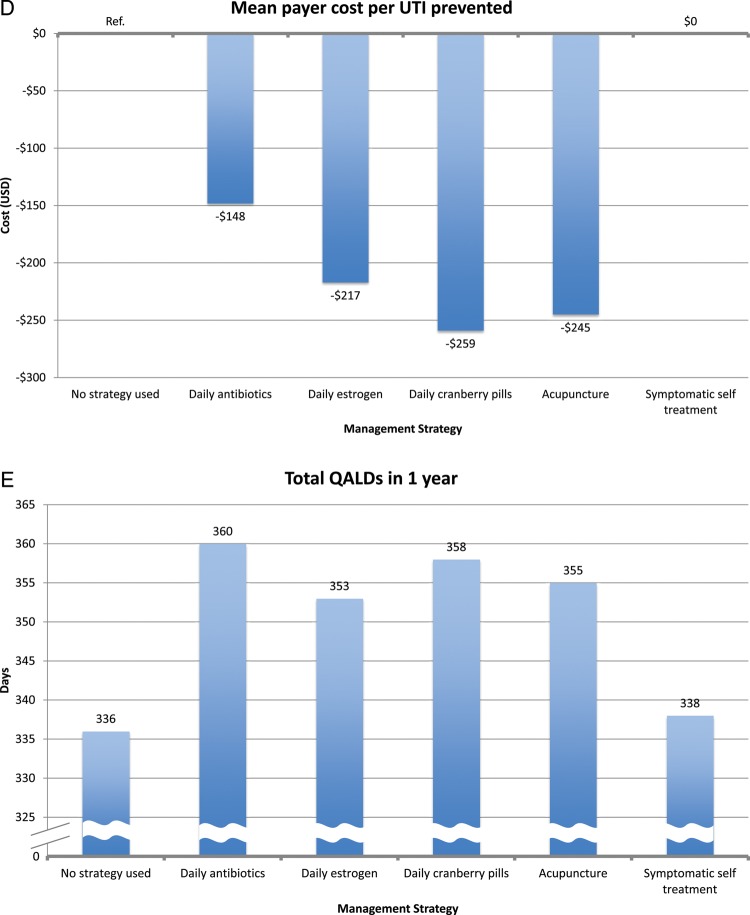
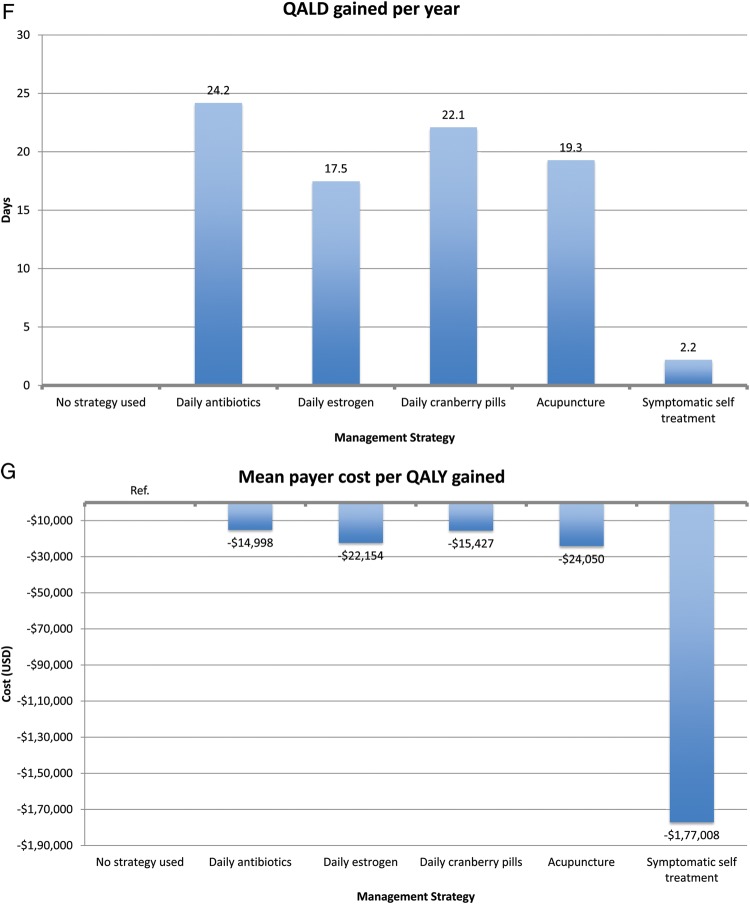
Results: Five strategies had ≥2 clinical trials published: (1) daily antibiotic (nitrofurantoin) prophylaxis; (2) daily estrogen prophylaxis; (3) daily cranberry prophylaxis; (4) acupuncture prophylaxis; and (5) symptomatic self-treatment. In the 3 UTIs/year model, nitrofurantoin prophylaxis was most effective, reducing the UTI rate to 0.4 UTIs/year, and the most expensive to the payer ($821/year). All other strategies resulted in payer cost savings but were less efficacious. Symptomatic self-treatment was the only strategy that resulted in patient cost savings, and was the most favorable strategy in term of cost per quality-adjusted life-year (QALY) gained.
Conclusions: Daily antibiotic use is the most effective strategy for recurrent UTI prevention compared to daily cranberry pills, daily estrogen therapy, and acupuncture. Cost savings to payers and patients were seen for most regimens, and improvement in QALYs were seen with all. Our findings provide clinically meaningful data to guide the physician-patient partnership in determining a preferred method of prevention for this common clinical problem.
Keywords: management; recurrent; urinary tract infection.
Figures
Comment in
-
Editorial commentary: including the X-factor: toward patient-centered prevention of urinary tract infection.Clin Infect Dis. 2014 Jan;58(2):161-3. doi: 10.1093/cid/cit648. Epub 2013 Sep 24. Clin Infect Dis. 2014. PMID: 24065332 No abstract available.
References
-
- Foxman B, Barlow R, D'Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs. Ann Epidemiol. 2000;10:509–15. - PubMed
-
- Griebling TL. Urologic diseases in America project: trends in resource use for urinary tract infections in women. J Urol. 2005;173:1281–7. - PubMed
-
- Kozak LJ, DeFrances CJ, Hall MJ. National hospital discharge survey: 2004 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13. 2006(Oct):1–209. - PubMed
-
- National Kidney and Urologic Diseases Information Clearinghouse. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases; 2010. Kidney and urologic diseases statistics for the United States.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
