

First-in-human, pharmacokinetic and pharmacodynamic phase I study of Resminostat, an oral histone deacetylase inhibitor, in patients with advanced solid tumors
- PMID: 24065624
- PMCID: PMC3790647
- DOI: 10.1158/1078-0432.CCR-13-0735
First-in-human, pharmacokinetic and pharmacodynamic phase I study of Resminostat, an oral histone deacetylase inhibitor, in patients with advanced solid tumors
Abstract
Purpose: This first-in-human dose-escalating trial investigated the safety, tolerability, maximum tolerated dose (MTD), dose-limiting toxicities (DLT), pharmacokinetics, and pharmacodynamics of the novel histone deacetylase (HDAC) inhibitor resminostat in patients with advanced solid tumors.
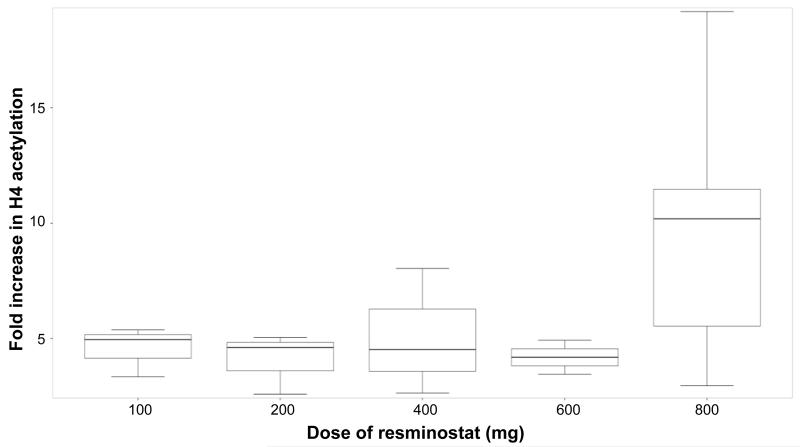
Experimental design: Resminostat was administered orally once-daily on days 1 to 5 every 14 days at 5 dose levels between 100 and 800 mg. Safety, pharmacokinetics, pharmacodynamics including histone acetylation and HDAC enzyme activity, and antitumor efficacy were assessed.
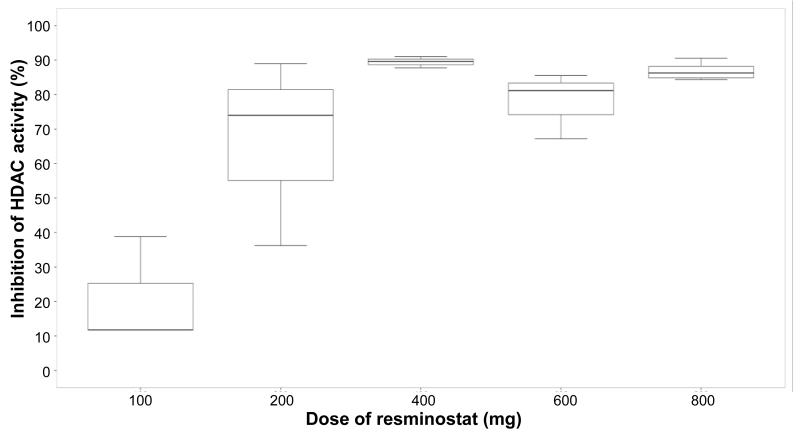
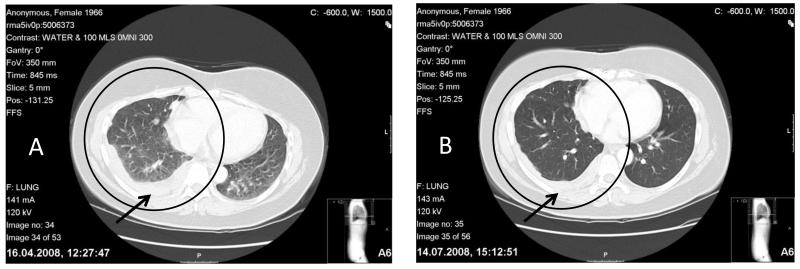
Results: Nineteen patients (median age 58 years, range 39-70) were treated. At 800 mg, 1 patient experienced grade 3 nausea and vomiting, grade 2 liver enzyme elevation, and grade 1 hypokalemia and thrombocytopenia; these were declared as a combined DLT. No other DLT was observed. Although an MTD was not reached and patients were safely dosed up to 800 mg, 3 of 7 patients treated with 800 mg underwent dose reductions after the DLT-defining period due to cumulative gastrointestinal toxicities and fatigue. All toxicities resolved following drug cessation. No grade 4 treatment-related adverse event was observed. The pharmacokinetic profile was dose-proportional with low inter-patient variability. Pharmacodynamic inhibition of HDAC enzyme was dose-dependent and reached 100% at doses ≥400 mg. Eleven heavily pretreated patients had stable disease and 1 patient with metastatic thymoma had a 27% reduction in target lesion dimensions.
Conclusions: Resminostat was safely administered with a dose-proportional pharmacokinetic profile, optimal on-target pharmacodynamic activity at dose levels ≥400 mg and signs of antitumor efficacy. The recommended phase II dose is 600 mg once-daily on days 1 to 5 every 14 days.
Figures
References
-
- Bolden JE, Peart MJ, Johnstone RW. Anticancer activities of histone deacetylase inhibitors. Nat Rev Drug Discov. 2006;5:769–84. - PubMed
-
- Gray SG, Qian CN, Furge K, Guo X, Teh BT. Microarray profiling of the effects of histone deacetylase inhibitors on gene expression in cancer cell lines. Int J Oncol. 2004;24:773–95. - PubMed
-
- Workman JL, Kingston RE. Alteration of nucleosome structure as a mechanism of transcriptional regulation. Annu Rev Biochem. 1998;67:545–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
