

Iron deposition following chronic myocardial infarction as a substrate for cardiac electrical anomalies: initial findings in a canine model
- PMID: 24066038
- PMCID: PMC3774668
- DOI: 10.1371/journal.pone.0073193
Iron deposition following chronic myocardial infarction as a substrate for cardiac electrical anomalies: initial findings in a canine model
Abstract
Purpose: Iron deposition has been shown to occur following myocardial infarction (MI). We investigated whether such focal iron deposition within chronic MI lead to electrical anomalies.
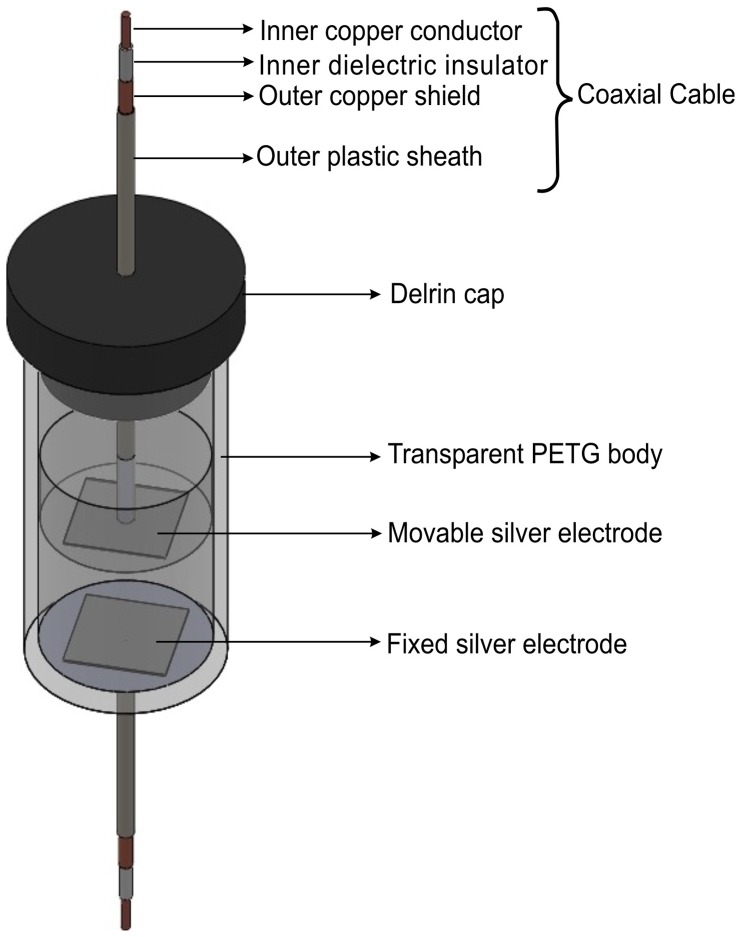
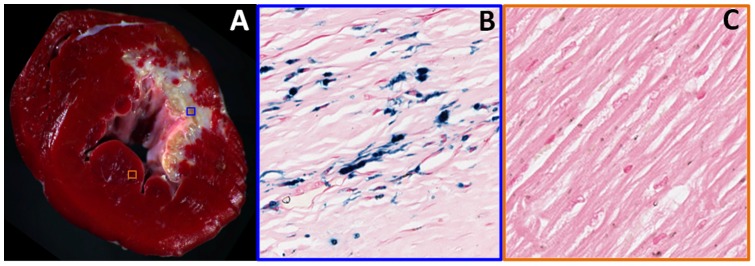
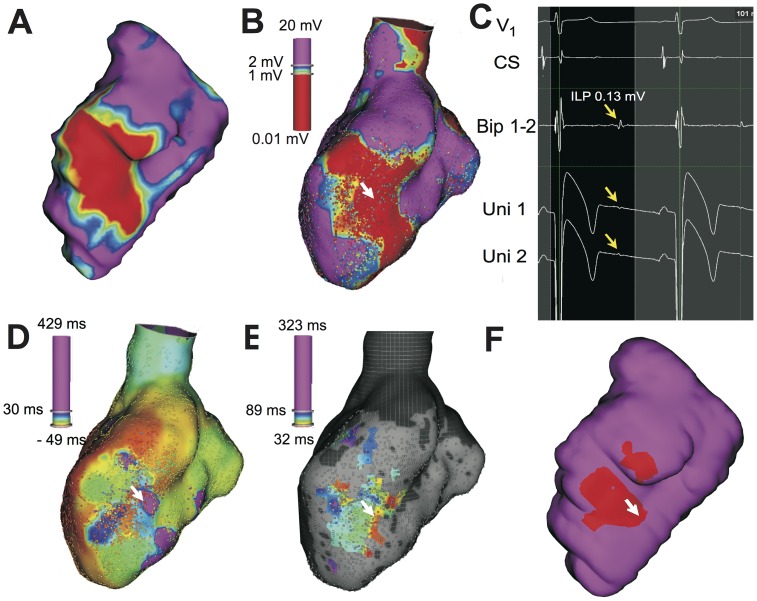
Methods: Two groups of dogs (ex-vivo (n = 12) and in-vivo (n = 10)) were studied at 16 weeks post MI. Hearts of animals from ex-vivo group were explanted and sectioned into infarcted and non-infarcted segments. Impedance spectroscopy was used to derive electrical permittivity ([Formula: see text]) and conductivity ([Formula: see text]). Mass spectrometry was used to classify and characterize tissue sections with (IRON+) and without (IRON-) iron. Animals from in-vivo group underwent cardiac magnetic resonance imaging (CMR) for estimation of scar volume (late-gadolinium enhancement, LGE) and iron deposition (T2*) relative to left-ventricular volume. 24-hour electrocardiogram recordings were obtained and used to examine Heart Rate (HR), QT interval (QT), QT corrected for HR (QTc) and QTc dispersion (QTcd). In a fraction of these animals (n = 5), ultra-high resolution electroanatomical mapping (EAM) was performed, co-registered with LGE and T2* CMR and were used to characterize the spatial locations of isolated late potentials (ILPs).
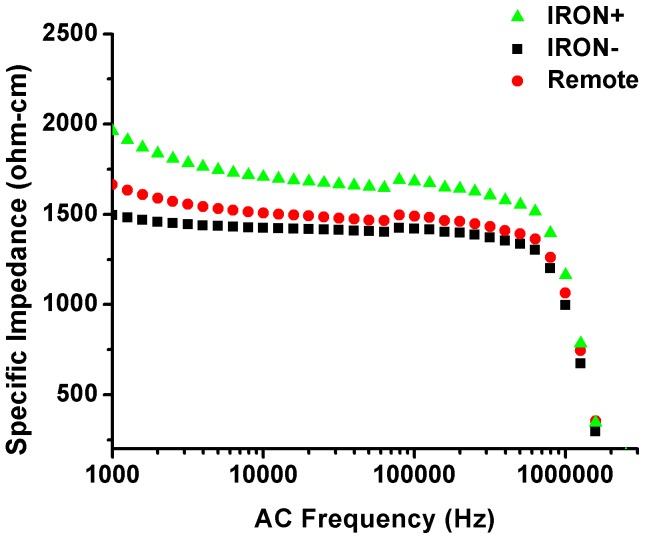
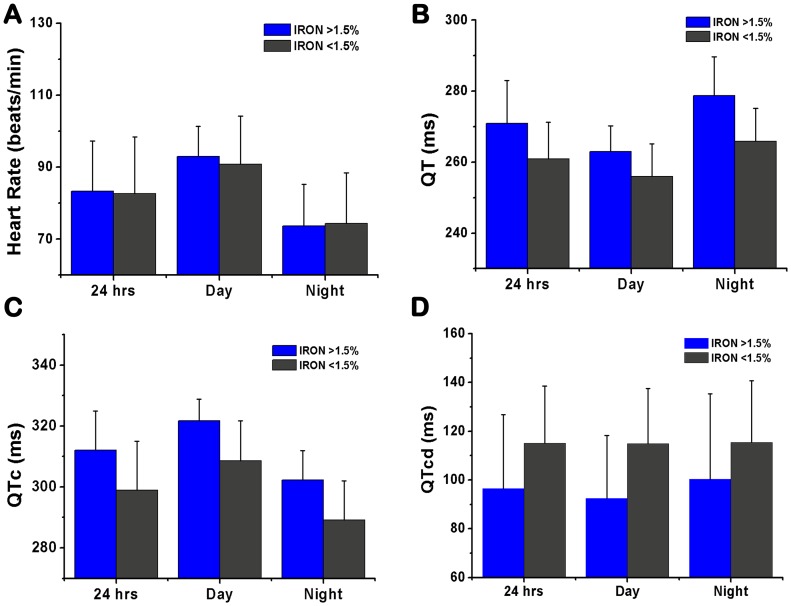
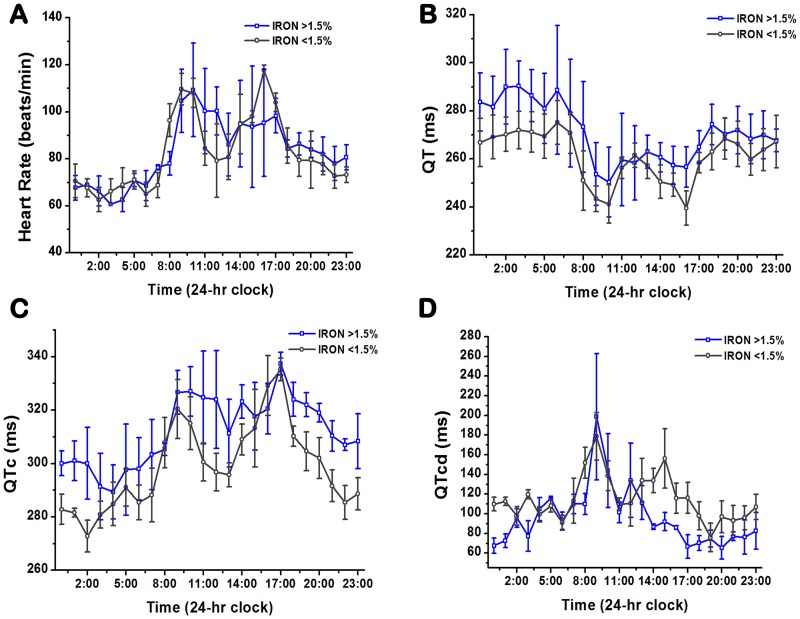
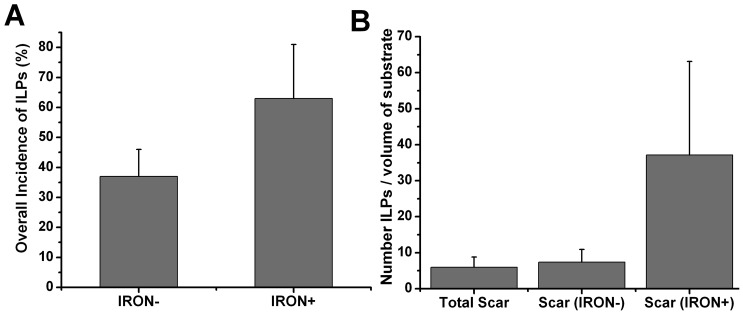
Results: Compared to IRON- sections, IRON+ sections had higher[Formula: see text], but no difference in[Formula: see text]. A linear relationship was found between iron content and [Formula: see text] (p<0.001), but not [Formula: see text] (p = 0.34). Among two groups of animals (Iron (<1.5%) and Iron (>1.5%)) with similar scar volumes (7.28% ± 1.02% (Iron (<1.5%)) vs 8.35% ± 2.98% (Iron (>1.5%)), p = 0.51) but markedly different iron volumes (1.12% ± 0.64% (Iron (<1.5%)) vs 2.47% ± 0.64% (Iron (>1.5%)), p = 0.02), QT and QTc were elevated and QTcd was decreased in the group with the higher iron volume during the day, night and 24-hour period (p<0.05). EAMs co-registered with CMR images showed a greater tendency for ILPs to emerge from scar regions with iron versus without iron.
Conclusion: The electrical behavior of infarcted hearts with iron appears to be different from those without iron. Iron within infarcted zones may evolve as an arrhythmogenic substrate in the post MI period.
Conflict of interest statement
Figures
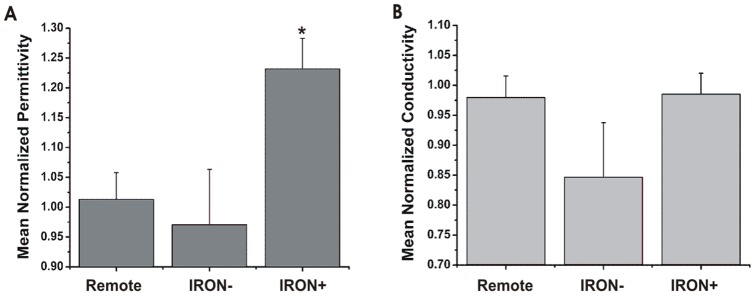
 measured from Remote, IRON−, and IRON+ infarct sections showed significantly greater
measured from Remote, IRON−, and IRON+ infarct sections showed significantly greater  (*, p<0.001) in IRON+ compared to Remote and IRON− sections; (B) however, mean
(*, p<0.001) in IRON+ compared to Remote and IRON− sections; (B) however, mean  measured from Remote, IRON−, and IRON+ infarct sections did not show any statistical difference in
measured from Remote, IRON−, and IRON+ infarct sections did not show any statistical difference in  between the different sections.
between the different sections.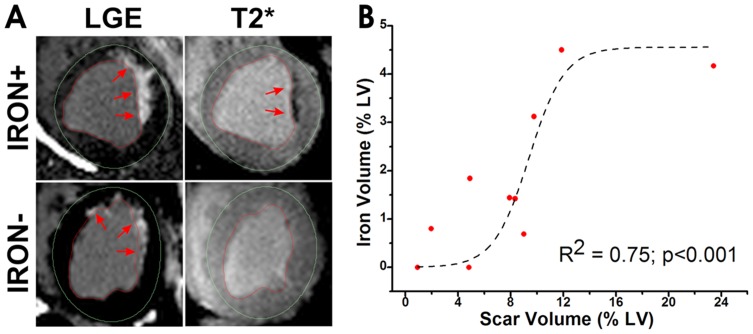
References
-
- Issa ZF, Miller JM, Zipes DP (2012) Clinical arrhythmology and electrophysiology: a companion to Braunwald's heart disease. Philadelphia, Pa; London: Saunders.
-
- Shenasa M (2013) Cardiac mapping. ChichesterWest Sussex; HobokenNJ: Wiley-Blackwell. xx, 945 p.
-
- de Bakker JM, van Capelle FJ, Janse MJ, Wilde AA, Coronel R, et al. (1988) Reentry as a cause of ventricular tachycardia in patients with chronic ischemic heart disease: electrophysiologic and anatomic correlation. Circulation 77: 589–606. - PubMed
-
- de Bakker JM, Coronel R, Tasseron S, Wilde AA, Opthof T, et al. (1990) Ventricular tachycardia in the infarcted, Langendorff-perfused human heart: role of the arrangement of surviving cardiac fibers. J Am Coll Cardiol 15: 1594–1607. - PubMed
-
- Cinca J, Bardaji A, Carreno A, Mont L, Bosch R, et al. (1995) ST segment elevation at the surface of a healed transmural myocardial infarction in pigs. Conditions for passive transmission from the ischemic peri-infarction zone. Circulation 91: 1552–1559. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
