

Task-sharing of HIV care and ART initiation: evaluation of a mixed-care non-physician provider model for ART delivery in rural Malawi
- PMID: 24066099
- PMCID: PMC3774791
- DOI: 10.1371/journal.pone.0074090
Task-sharing of HIV care and ART initiation: evaluation of a mixed-care non-physician provider model for ART delivery in rural Malawi
Abstract
Background: Expanding access to antiretroviral therapy (ART) in sub-Saharan Africa requires implementation of alternative care delivery models to traditional physician-centered approaches. This longitudinal analysis compares outcomes of patients initiated on antiretroviral therapy (ART) by non-physician and physician providers.
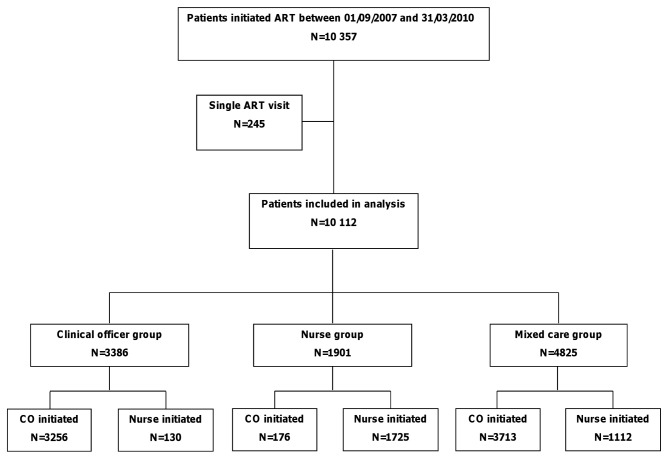
Methods: Adults (≥15 years) initiating ART between September 2007 and March 2010, and with >1 follow-up visit were included and classified according to the proportion of clinical visits performed by nurses or by clinical officers (≥ 80% of visits). Multivariable Poisson models were used to compare 2-year program attrition (mortality and lost to follow-up) and mortality by type of provider. In sensitivity analyses only patients with less severe disease were included.
Results: A total of 10,112 patients contributed 14,012 person-years to the analysis: 3386 (33.5%) in the clinical officer group, 1901 (18.8%) in the nurse care group and 4825 (47.7%) in the mixed care group. Overall 2-year program retention was 81.8%. Attrition was lower in the mixed care and higher in the clinical officer group, compared to the nurse group (adjusted incidence rate ratio [aIRR]=0.54, 95%CI 0.45-0.65; and aIRR=3.03, 95%CI 2.56-3.59, respectively). While patients initiated on ART by clinical officers in the mixed care group had lower attrition (aIRR=0.36, 95%CI 0.29-0.44) than those in the overall nurse care group; no differences in attrition were found between patients initiated on ART by nurses in the mixed care group and those included in the nurse group (aIRR=1.18, 95%CI 0.95-1.47). Two-year mortality estimates were aIRR=0.72, 95%CI 0.49-1.09 and aIRR=5.04, 95%CI 3.56-7.15, respectively. Slightly higher estimates were observed when analyses were restricted to patients with less severe disease.
Conclusion: The findings of this study support the use of a mixed care model with well trained and regularly supervised nurses and medical assistants to provide HIV care in countries with high HIV prevalence.
Conflict of interest statement
Figures
References
-
- Joint United Nations Programme on HIV/AIDS (2010) UNAIDS report on the global AIDS epidemic 2010. Available: http://www.unaids.org/globalreport/. Accessed 5 August 2013.
-
- Bartlett JA, Shao JF (2009) Successes, challenges, and limitations of current antiretroviral therapy in low-income and middle-income countries. Lancet Infect Dis 9: 637-649. doi:10.1016/S1473-3099(09)70227-0. PubMed: 19778766. - DOI - PubMed
-
- Bärnighausen T, Bloom DE, Humair S (2007) Human resources for treating HIV/AIDS: needs, capacities, and gaps. AIDS Patient Care STDs 21: 799-812. doi:10.1089/apc.2007.0193. PubMed: 17944556. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
