

Challenges and opportunities for cancer vaccines in the current NSCLC clinical scenario
- PMID: 24066886
- PMCID: PMC4104452
- DOI: 10.2174/15680266113136660182
Challenges and opportunities for cancer vaccines in the current NSCLC clinical scenario
Abstract
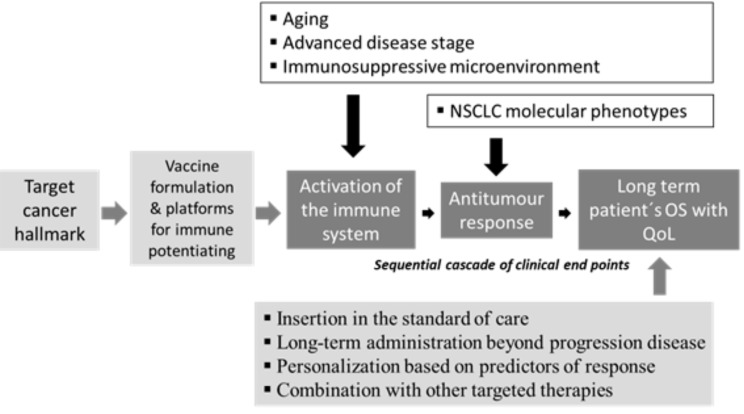
This review is aimed to focus on NSCLC as an emerging and promising model for active immunotherapy and the challenges for its inclusion in the current clinical scenario. Cancer vaccines for NSCLC have been focused as a therapeutic option based on the identification of a tumor hallmark and the active immunization with the related molecules that triggers cellular and/or humoral responses that consequently destroy or delay the rate of malignant progression. This therapeutic intervention in an established disease state has been aimed to impact into prolonging patient´s survival with ethically accepted quality of life. Understanding of relationship between structure and function in cancer vaccines is essential to interpret their opportunities to impact into prolonging survival and increasing quality of life in cancer patients. It is widely accepted that the failure of the cancer vaccines in the NSCLC scenario is related with its introduction in the advanced disease stages and poor performance status of the patients due to the combination of the tumor induced immunosuppression with the immune senescence. Despite first, second and emerging third line of onco-specific treatments the life expectancy for NSCLC patients diagnosed at advanced stages is surrounding the 12 months of median survival and in facts the today real circumstances are extremely demanding for the success inclusion of cancer vaccines as therapeutic choice in the clinical scenario. The kinetics of the active immunizations encompasses a sequential cascade of clinical endpoints: starting by the activation of the immune system, followed by the antitumor response and finalizing with the consequential impact on patients' overall survival. Today this cascade of clinical endpoints is the backbone for active immunization assessment and moreover the concept of cancer vaccines, applied in the NSCLC setting, is just evolving as a complex therapeutic strategy, in which the opportunities for cancer vaccines start from the selection of the target cancer hallmark, followed by the vaccine formulation and its platforms for immune potentiating, also cover the successful insertion in the standard of care, the chronic administration beyond progression disease, the personalization based on predictors of response and the potential combination with other targeted therapies.
Figures
References
-
- Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell. 2011;144:646–74. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
