

Ascorbate infusion increases skeletal muscle fatigue resistance in patients with chronic obstructive pulmonary disease
- PMID: 24068051
- PMCID: PMC3841801
- DOI: 10.1152/ajpregu.00360.2013
Ascorbate infusion increases skeletal muscle fatigue resistance in patients with chronic obstructive pulmonary disease
Abstract
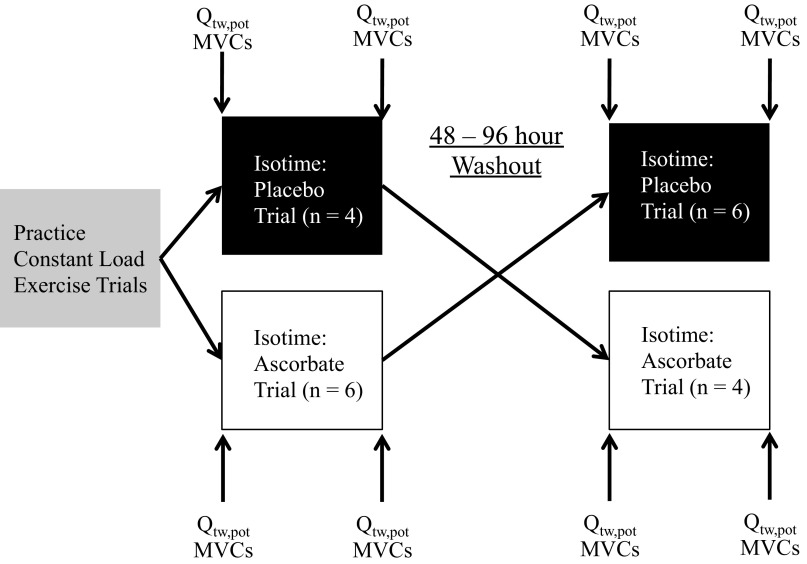
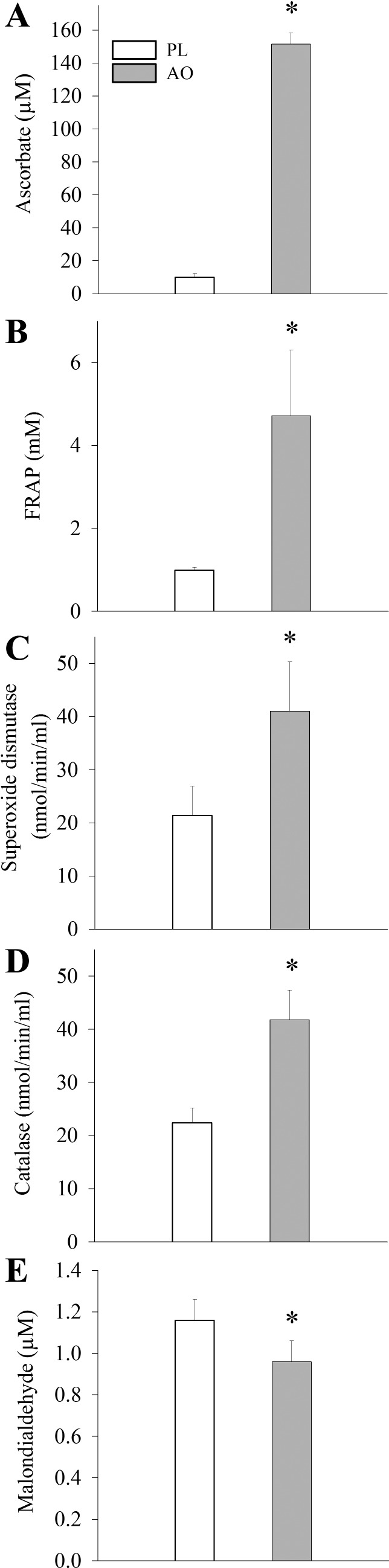
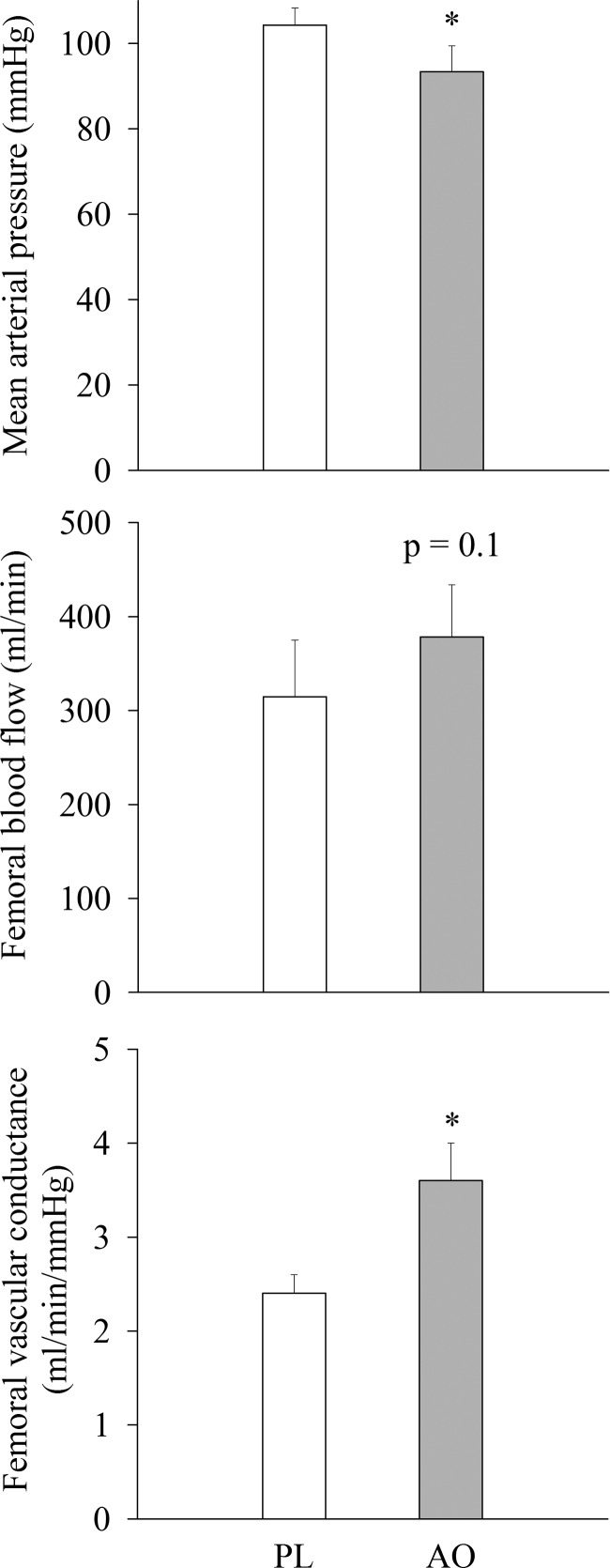
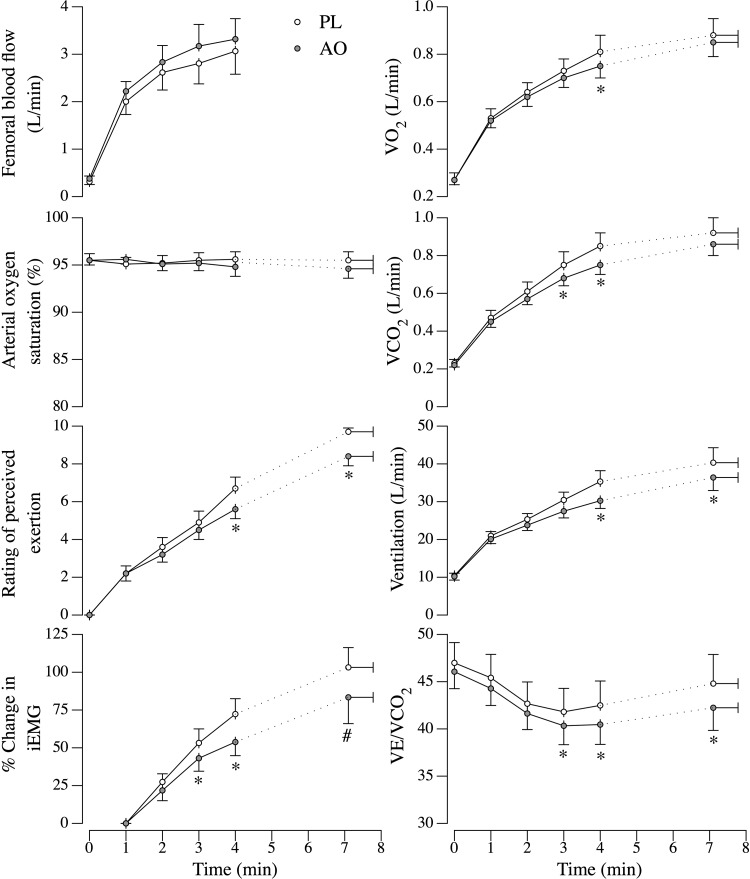
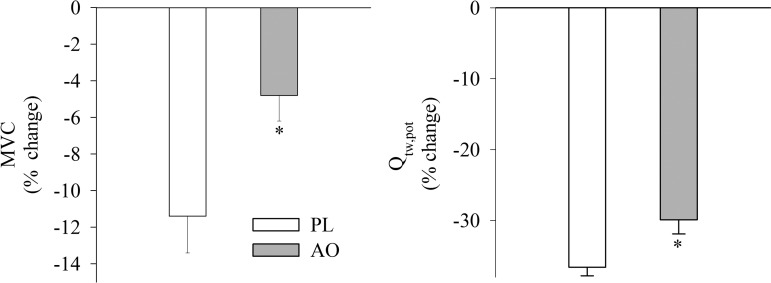
Chronic obstructive pulmonary disease (COPD) is associated with systemic oxidative stress and skeletal muscle dysfunction. The purpose of this study was to examine the impact of intravenous ascorbate administration (AO) on biological markers of antioxidant capacity and oxidative stress, and subsequently skeletal muscle function during dynamic, small muscle mass exercise in patients with COPD. Ten patients with spirometric evidence of COPD performed single-leg knee extensor (KE) trials matched for intensity and time (isotime) following intravenous ascorbate (2 g) or saline infusion (PL). Quadriceps fatigue was quantified by changes in force elicited by maximal voluntary contraction (MVC) and magnetic femoral nerve stimulation (Qtw,pot). AO administration significantly increased antioxidant capacity, as measured by the ferric-reducing ability of plasma (PL: 1 ± 0.1 vs. AO: 5 ± 0.2 mM), and significantly reduced malondialdehyde levels (PL: 1.16 ± 0.1 vs. AO: 0.97 ± 0.1 mmol). Additionally, resting blood pressure was significantly reduced (PL: 104 ± 4 vs. AO: 93 ± 6 mmHg) and resting femoral vascular conductance was significantly elevated after AO (PL: 2.4 ± 0.2 vs. AO: 3.6 ± 0.4 ml·min(-1)·mmHg(-1)). During isotime exercise, the AO significantly attenuated both the ventilatory and metabolic responses, and patients accumulated significantly less peripheral quadriceps fatigue, as illustrated by less of a fall in MVC (PL: -11 ± 2% vs. AO: -5 ± 1%) and Qtw,pot (PL: -37 ± 1% vs. AO: -30 ± 2%). These data demonstrate a beneficial role of AO administration on skeletal muscle fatigue in patients with COPD and further implicate systemic oxidative stress as a causative factor in the skeletal muscle dysfunction observed in this population.
Keywords: ascorbate; free radicals; peripheral fatigue.
Figures
Similar articles
-
Oxidative stress and COPD: the effect of oral antioxidants on skeletal muscle fatigue.Med Sci Sports Exerc. 2013 Jul;45(7):1235-43. doi: 10.1249/MSS.0b013e3182846d7e. Med Sci Sports Exerc. 2013. PMID: 23299763 Free PMC article. Clinical Trial.
-
Ascorbate attenuates cycling exercise-induced neuromuscular fatigue but fails to improve exertional dyspnea and exercise tolerance in COPD.J Appl Physiol (1985). 2021 Jan 1;130(1):69-79. doi: 10.1152/japplphysiol.00611.2020. Epub 2020 Nov 5. J Appl Physiol (1985). 2021. PMID: 33151775 Free PMC article.
-
Antioxidants and aging: NMR-based evidence of improved skeletal muscle perfusion and energetics.Am J Physiol Heart Circ Physiol. 2009 Nov;297(5):H1870-5. doi: 10.1152/ajpheart.00709.2009. Epub 2009 Sep 18. Am J Physiol Heart Circ Physiol. 2009. PMID: 19767527 Free PMC article. Clinical Trial.
-
The role of active muscle mass in determining the magnitude of peripheral fatigue during dynamic exercise.Am J Physiol Regul Integr Comp Physiol. 2014 Jun 15;306(12):R934-40. doi: 10.1152/ajpregu.00043.2014. Epub 2014 Apr 16. Am J Physiol Regul Integr Comp Physiol. 2014. PMID: 24740653 Free PMC article.
-
Skeletal muscle dysfunction in patients with chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2008;3(4):637-58. doi: 10.2147/copd.s4480. Int J Chron Obstruct Pulmon Dis. 2008. PMID: 19281080 Free PMC article. Review.
Cited by
-
COPD: balancing oxidants and antioxidants.Int J Chron Obstruct Pulmon Dis. 2015 Feb 2;10:261-76. doi: 10.2147/COPD.S42414. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 25673984 Free PMC article. Review.
-
Skeletal muscle mitochondrial adaptations induced by long-term cigarette smoke exposure.Am J Physiol Endocrinol Metab. 2021 Jul 1;321(1):E80-E89. doi: 10.1152/ajpendo.00544.2020. Epub 2021 Jun 14. Am J Physiol Endocrinol Metab. 2021. PMID: 34121449 Free PMC article.
-
Reduced HDAC2 in skeletal muscle of COPD patients.Respir Res. 2017 May 19;18(1):99. doi: 10.1186/s12931-017-0588-8. Respir Res. 2017. PMID: 28526090 Free PMC article.
-
Quadriceps exercise intolerance in patients with chronic obstructive pulmonary disease: the potential role of altered skeletal muscle mitochondrial respiration.J Appl Physiol (1985). 2015 Oct 15;119(8):882-8. doi: 10.1152/japplphysiol.00460.2015. Epub 2015 Aug 13. J Appl Physiol (1985). 2015. PMID: 26272320 Free PMC article.
-
Endothelial function is impaired in the cutaneous microcirculation of adults with psoriasis through reductions in nitric oxide-dependent vasodilation.Am J Physiol Heart Circ Physiol. 2018 Feb 1;314(2):H343-H349. doi: 10.1152/ajpheart.00446.2017. Epub 2017 Oct 20. Am J Physiol Heart Circ Physiol. 2018. PMID: 29054972 Free PMC article.
References
-
- Allen DG, Lamb GD, Westerblad H. Skeletal muscle fatigue: cellular mechanisms. Physiol Rev 88: 287–332, 2008 - PubMed
-
- Amann M, Calbet JA. Convective oxygen transport and fatigue. J Appl Physiol 104: 861–870, 2008 - PubMed
-
- Benzie IF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: the FRAP assay. Anal Biochem 239: 70–76, 1996 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous