

Preterm birth and mortality and morbidity: a population-based quasi-experimental study
- PMID: 24068297
- PMCID: PMC3823714
- DOI: 10.1001/jamapsychiatry.2013.2107
Preterm birth and mortality and morbidity: a population-based quasi-experimental study
Abstract
Importance: Preterm birth is associated with increased mortality and morbidity. However, previous studies have been unable to rigorously examine whether confounding factors cause these associations rather than the harmful effects of being born preterm.
Objective: To estimate the extent to which the associations between early gestational age and offspring mortality and morbidity are the result of confounding factors by using a quasi-experimental design, the sibling-comparison approach, and by controlling for statistical covariates that varied within families.
Design, setting, and participants: A population-based cohort study, combining Swedish registries to identify all individuals born in Sweden from 1973 to 2008 (3,300,708 offspring of 1,736,735 mothers) and link them with multiple outcomes.
Main outcomes and measures: Offspring mortality (during infancy and throughout young adulthood) and psychiatric (psychotic or bipolar disorder, autism, attention-deficit/hyperactivity disorder, suicide attempts, substance use, and criminality), academic (failing grades and educational attainment), and social (partnering, parenthood, low income, and social welfare benefits) outcomes through 2009.
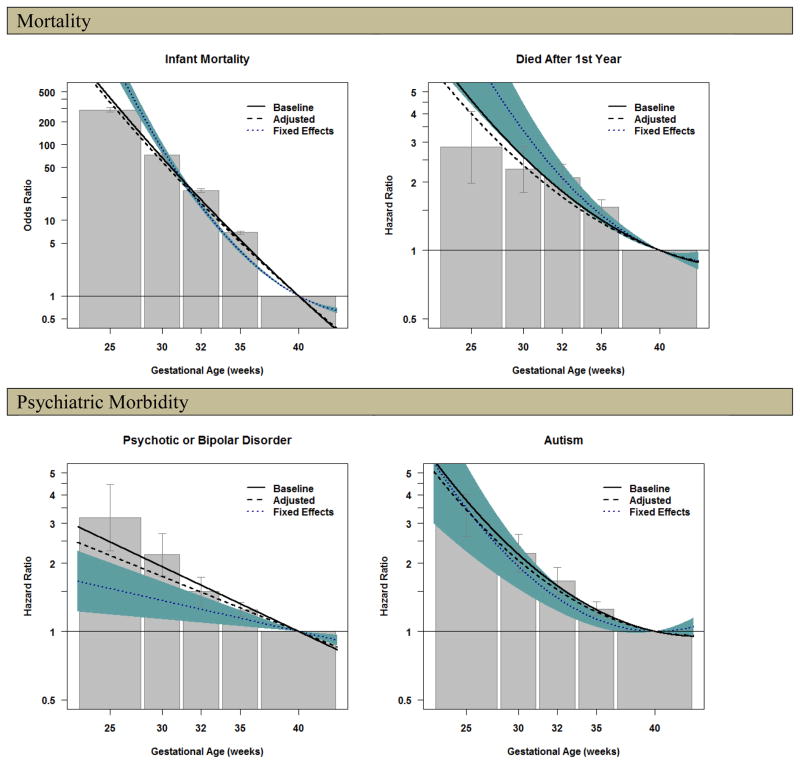
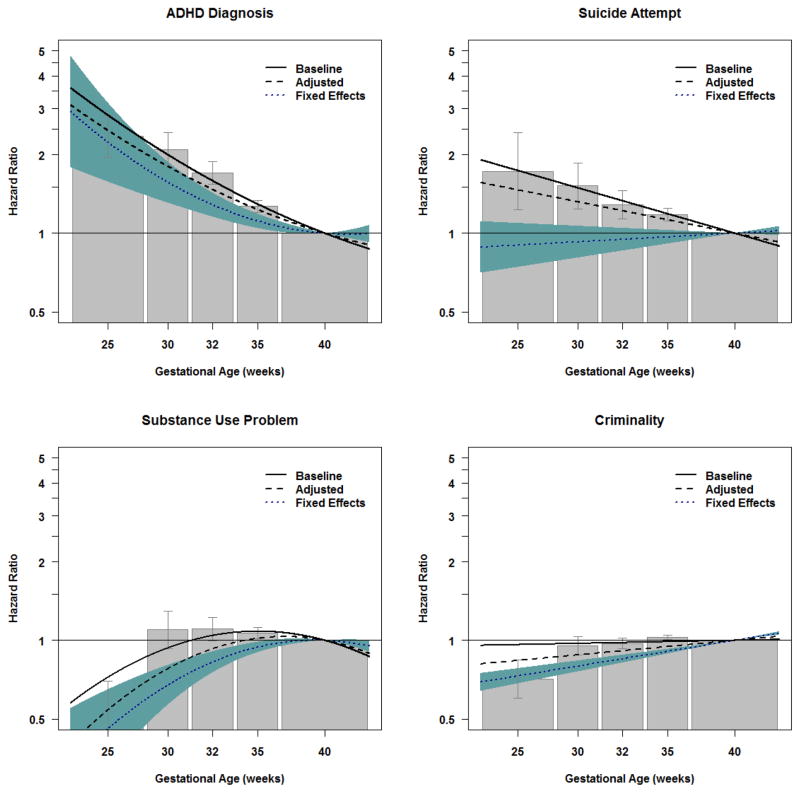
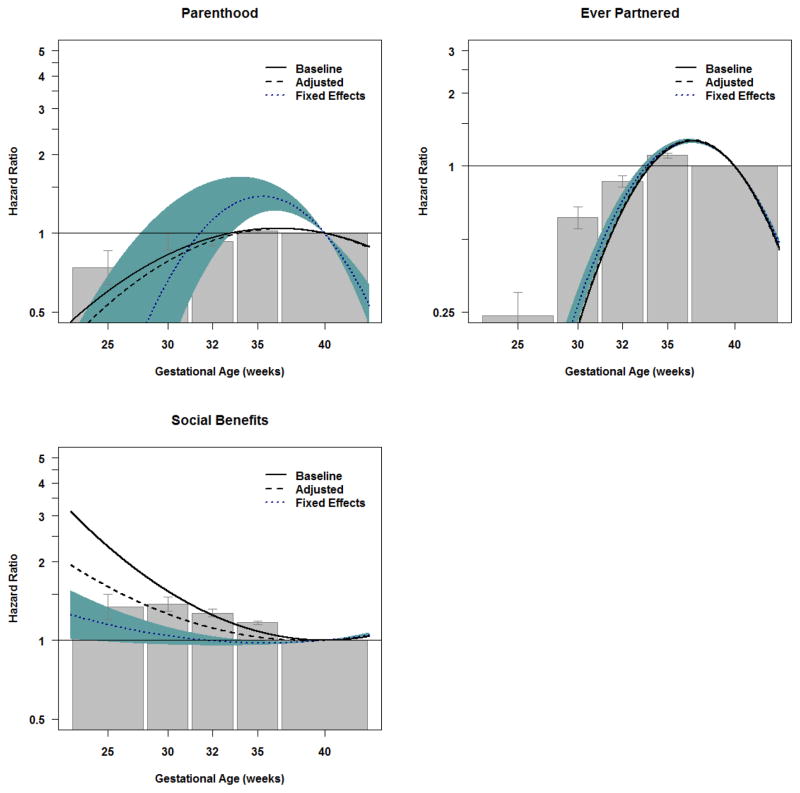
Results: In the population, there was a dose-response relationship between early gestation and the outcome measures. For example, extreme preterm birth (23-27 weeks of gestation) was associated with infant mortality (odds ratio, 288.1; 95% CI, 271.7-305.5), autism (hazard ratio [HR], 3.2; 95% CI, 2.6-4.0), low educational attainment (HR, 1.7; 1.5-2.0), and social welfare benefits (HR, 1.3; 1.2-1.5) compared with offspring born at term. The associations between early gestation and mortality and psychiatric morbidity generally were robust when comparing differentially exposed siblings and controlling for statistical covariates, whereas the associations with academic and some social problems were greatly or completely attenuated in the fixed-effects models.
Conclusions and relevance: The mechanisms responsible for the associations between preterm birth and mortality and morbidity are outcome-specific. Associations between preterm birth and mortality and psychiatric morbidity are largely independent of shared familial confounds and measured covariates, consistent with a causal inference. However, some associations, particularly predicting suicide attempt, educational attainment, and social welfare benefits, are the result of confounding factors. The findings emphasize the importance of both reducing preterm birth and providing wraparound services to all siblings in families with an offspring born preterm.
Conflict of interest statement
There were no financial or other conflicts of interest for any of the authors. Neither this manuscript nor one with substantially similar content under our authorship has been published or is being considered for publication elsewhere.
Figures
References
-
- EXPRESS Group members. One-year survival of extremely preterm infants after active perinatal care in Sweden. JAMA. 2009;301:2225–2233. - PubMed
-
- Moster D, Terje L, Markestad T. Long-term medical and social consequences of preterm birth. The New England Journal of Medicine. 2008;359:262–273. - PubMed
-
- Crump C, Sundquist K, Sundquist J, Winkleby MA. Gestational age at birth and mortality in young adulthood. JAMA. 2011;306:1233–1240. - PubMed
-
- Doyle LW, Anderson PJ. Adult outcome of extremely preterm infants. Pediatrics. 2010;126:342–351. - PubMed
-
- McCormick MC, Litt JS, Smith VC, Zupancic JAF. Prematurity: An overview and public health implications. Annual Review Public Health. 2011;32:367–379. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
