

Pediatric non-alcoholic fatty liver disease: an increasing public health issue
- PMID: 24068459
- PMCID: PMC3929043
- DOI: 10.1007/s00431-013-2157-6
Pediatric non-alcoholic fatty liver disease: an increasing public health issue
Abstract
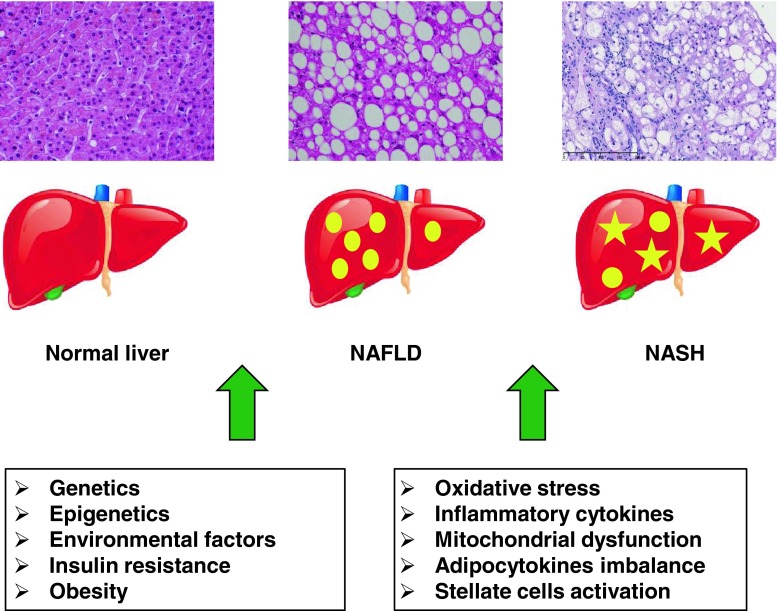
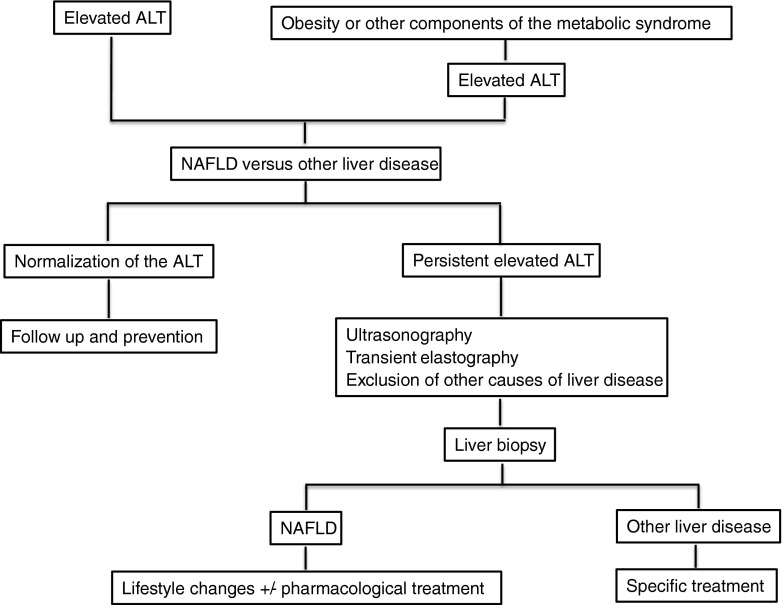
Non-alcoholic fatty liver disease (NAFLD) is a multifactorial condition that encompasses a wide spectrum of liver abnormalities ranging from simple liver steatosis to steatohepatitis (non-alcoholic steatohepatitis), which may be associated with fibrosis and progress to cirrhosis and end-stage liver disease. NAFLD has recently become the most common cause of chronic liver disease in children and adolescents. NAFLD prevalence, alongside obesity, continues to increase among pediatric patients. Obesity is believed to represent a major risk factor for NAFLD, which is considered to be the liver presentation of the metabolic syndrome. Although the pathogenesis of NAFLD is not fully understood, the notion that multiple factors affect disease development and progression is widely accepted. Both genetic background and environmental factors contribute to NAFLD development. A more complete understanding of the pathogenesis may aid in developing non-invasive diagnostic tools and identifying new therapeutic targets. Liver biopsy currently remains the gold standard for NAFLD diagnosis and staging. Although lifestyle and diet modifications are key in NAFLD treatment, the development of new pharmacological therapies is crucial for patients who are unresponsive to first-line therapy.
Conclusion: Pediatric NAFLD is an increasing public health issue that remains underdiagnosed. A large-scale screening in the high-risk population, especially among the overweight pediatric patients, should be considered, including measurement of serum transaminases and liver ultrasound. It is crucial to treat this condition as soon as possible in order to avoid the progression to end-stage liver disease.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
