

Impact of corticofugal fibre involvement in subcortical stroke
- PMID: 24068765
- PMCID: PMC3787414
- DOI: 10.1136/bmjopen-2013-003318
Impact of corticofugal fibre involvement in subcortical stroke
Abstract
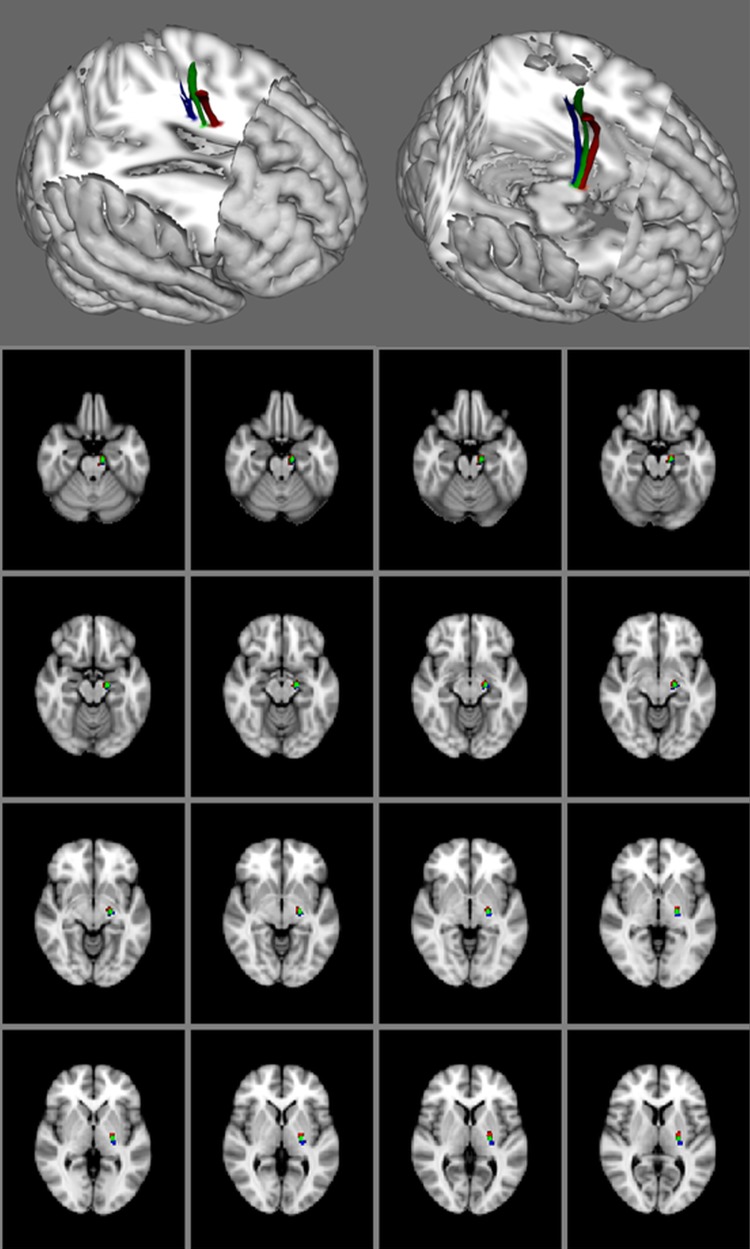
Objective: To correlate motor deficit with involvement of corticofugal fibres in patients with subcortical stroke. The descending motor corticofugal fibres originate from the primary motor cortex (M1), dorsal and ventral premotor area (PMdv) and supplementary motor area (SMA).
Design: Retrospective study.
Setting: Single tertiary teaching hospital.
Participants: 57 patients (57% men) with subcortical infarcts on MRI (2009-2011) were included. The mean age was 64.3±14.4 years.
Interventions: None.
Primary and secondary outcome measures: National Institute of Health Stroke Scale subscores for arm and leg motor deficit at 90 days.
Results: An area under the receiver operating characteristics curve (AUC) for the volume of overlap with infarct (and M1/PMdv/SMA fibres) and motor outcome was calculated. The AUC for the association with arm motor deficit from M1 fibres involvement was 0.80 (95% CI 0.66 to 0.94), PMdv was 0.76 (95% CI 0.61 to 0.91) and SMA was 0.73 (95% CI 0.58 to 0.88). The AUC for leg motor deficit from M1 fibres involvement was 0.69 (95% CI 0.52 to 0.85), PMdv was 0.67 (95% CI 0.50 to 0.85), SMA was 0.66 (95% CI 0.48 to 0.84).
Conclusions: Following subcortical stroke, the correlations between involvement of the corticofugal fibres for upper and lower limbs motor deficit were variable. A poor motor outcome was not universal following subcortical stroke.
Keywords: Rehabilitation Medicine; Stroke Medicine.
Figures
Similar articles
-
Topographic Evolution of Anterior Cerebral Artery Infarction and Its Impact on Motor Impairment.Cerebrovasc Dis. 2022;51(2):248-258. doi: 10.1159/000519134. Epub 2021 Sep 30. Cerebrovasc Dis. 2022. PMID: 34592733
-
Motor and premotor cortices in subcortical stroke: proton magnetic resonance spectroscopy measures and arm motor impairment.Neurorehabil Neural Repair. 2013 Jun;27(5):411-20. doi: 10.1177/1545968312469835. Epub 2013 Jan 8. Neurorehabil Neural Repair. 2013. PMID: 23300210 Free PMC article.
-
Corticospinal Fibers With Different Origins Impact Motor Outcome and Brain After Subcortical Stroke.Stroke. 2020 Jul;51(7):2170-2178. doi: 10.1161/STROKEAHA.120.029508. Epub 2020 Jun 17. Stroke. 2020. PMID: 32568657
-
Microstructure and Genetic Polymorphisms: Role in Motor Rehabilitation After Subcortical Stroke.Front Aging Neurosci. 2022 Feb 1;14:813756. doi: 10.3389/fnagi.2022.813756. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35177977 Free PMC article. Review.
-
Activation likelihood estimation meta-analysis of motor-related neural activity after stroke.Neuroimage. 2012 Feb 1;59(3):2771-82. doi: 10.1016/j.neuroimage.2011.10.023. Epub 2011 Oct 17. Neuroimage. 2012. PMID: 22023742 Review.
Cited by
-
PREP2: A biomarker-based algorithm for predicting upper limb function after stroke.Ann Clin Transl Neurol. 2017 Oct 24;4(11):811-820. doi: 10.1002/acn3.488. eCollection 2017 Nov. Ann Clin Transl Neurol. 2017. PMID: 29159193 Free PMC article.
-
Structural connectivity analyses in motor recovery research after stroke.Ann Clin Transl Neurol. 2016 Jan 19;3(3):233-44. doi: 10.1002/acn3.278. eCollection 2016 Mar. Ann Clin Transl Neurol. 2016. PMID: 27042683 Free PMC article. Review.
-
Corticospinal premotor fibers facilitate complex motor control after stroke.Ann Clin Transl Neurol. 2024 Sep;11(9):2439-2449. doi: 10.1002/acn3.52159. Epub 2024 Jul 28. Ann Clin Transl Neurol. 2024. PMID: 39073030 Free PMC article.
References
-
- Lawrence ES, Coshall C, Dundas R, et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 2001;32:1279–84 - PubMed
-
- Dewey HM, Thrift AG, Mihalopoulos C, et al. Cost of stroke in Australia from a societal perspective: results from the North East Melbourne Stroke Incidence Study (NEMESIS). Stroke 2001;32:2409–16 - PubMed
-
- Saver JL, Johnston KC, Homer D, et al. Infarct volume as a surrogate or auxiliary outcome measure in ischemic stroke clinical trials. The RANTTAS Investigators. Stroke 1999;30:293–98 - PubMed
-
- Lovblad KO, Baird AE, Schlaug G, et al. Ischemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging correlate with clinical outcome. Ann Neurol 1997;42:164–70 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources