

The incidence and determinants of decubitus ulcers in hospital care: an analysis of routine quality management data at a university hospital
- PMID: 24069079
- PMCID: PMC3782025
- DOI: 10.3238/arztebl.2013.0550
The incidence and determinants of decubitus ulcers in hospital care: an analysis of routine quality management data at a university hospital
Abstract
Background: The incidence of decubitus ulcers is an established quality indicator for external quality assurance in the inpatient setting. Epidemiologic analyses of the frequency of, and risk factors for, decubitus ulcers in routine care are lacking.
Method: We analyzed routine decubitus-ulcer documentation data relating to all inpatients of the University Hospital of Dresden, Germany, from 2007 to 2011 (n = 246 162 patients). The prevalence and incidence of decubitus ulcers and demographic and illness-related risk factors for them were determined with the use of descriptive techniques and logistic regression models. The effort-to-benefit ratio of documenting decubitus ulcers in various care scenarios was calculated in terms of the number of additional patients to be documented for each patient with incident decubitus ulcer.
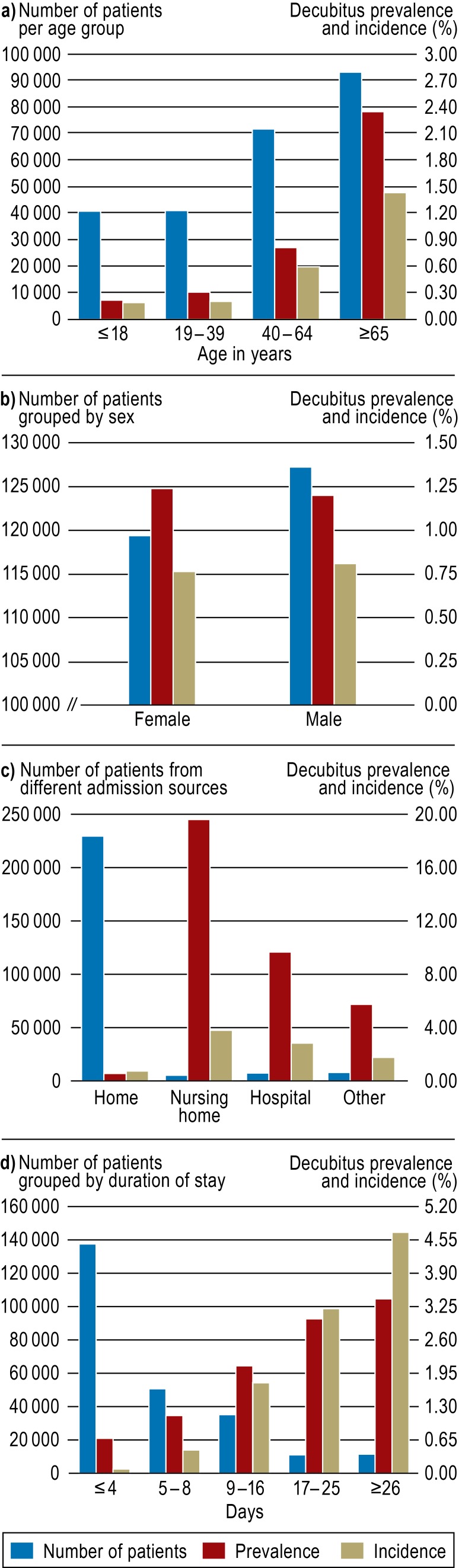
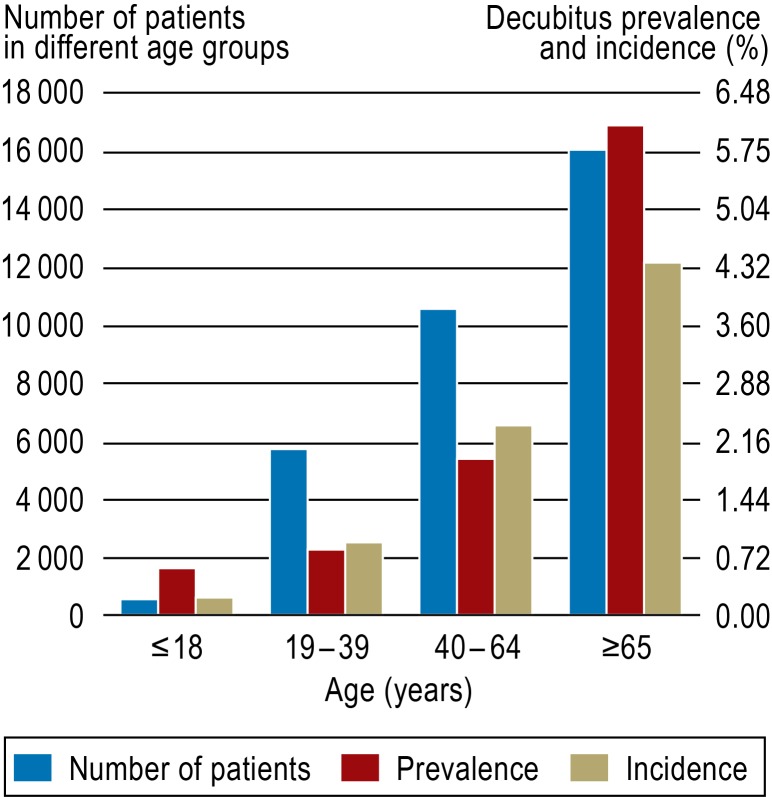
Results: The prevalence of decubitus ulcers was 1.21%, and their incidence during inpatient treatment was 0.78%, with significant differences across clinical care units (range of ward-specific incidences: 0.0% to 12.7%). Predictors for the development of a new decubitus ulcer during a hospital stay included higher age (odds ratio [OR] 1.03 per year, 95% confidence interval [CI] 1.02-1.03), longer hospital stay (OR 1.03 per day, 95% CI 1.031-1.033), treatment in an intensive care unit (OR 2.88, 95% CI 2.58-3.22), and transfer to the hospital from a residential nursing-care facility (OR 6.05, 95% CI 5.13-7.11). The patient's sex and the severity of disease were not correlated with the incidence of decubitus ulcers. The effort-to-benefit ratio could be improved if wards with a low incidence of decubitus ulcers (<0.5%) either entirely discontinued the current hospital-wide procedure for documenting decubitus ulcers (with one new ulcer for every 645 patients) or continued it only for patients aged 65 or older (with one new ulcer for every 902 patients).
Conclusion: There are major differences between clinical care units in the risk of decubitus ulcers. Epidemiological analysis of routine quality management data is useful to assess the benefit of measures taken in medical care. Continuing evaluation is essential.
Figures
References
-
- Fechner Björn-Ola. Indikatoren für die Bewertung von Komplikationsraten. Dtsch Arztebl. 2012;109(41):A 2026–A 2030.
-
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel 2009. European Pressure Ulcer Advisory Panel. www.epuap.org/guidelines/QRG_Prevention_in_German.pdf. (last accessed on 23 May 2012)
-
- European Pressure Ulcer Advisory Panel 2009. Leitlinie Dekubitus Prävention. Washington, DC. National Pressure Ulcer Advisory Panel. 2007
-
- Bienstein C, Schröder G, Braun M, Neander K-D. Stuttgart, New York: Thieme Verlag; 1997. Dekubitus: Die Herausforderung für Pflegende; pp. 42–63.
-
- Gesundheitsberichterstattung des Bundes. www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung.... pdf?__blob=publicationFile. Berlin: Robert-Koch-Institut; Dekubitus. (last accessed on 26 June 2013)
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical