

Meta-analysis of urine heme dipstick diagnosis of Schistosoma haematobium infection, including low-prevalence and previously-treated populations
- PMID: 24069486
- PMCID: PMC3772022
- DOI: 10.1371/journal.pntd.0002431
Meta-analysis of urine heme dipstick diagnosis of Schistosoma haematobium infection, including low-prevalence and previously-treated populations
Abstract
Background: Urogenital schistosomiasis remains highly endemic in Africa. Current control is based on drug administration, targeted either to school-age children or to high-risk communities at-large. Urine dipsticks for detection of microhematuria offer an inexpensive means for estimating infection prevalence. However, their diagnostic performance has not been systematically evaluated after community treatment, or in areas with continuing low prevalence. The objective of the present study was to perform meta-analysis of dipstick accuracy for S. haematobium infection in endemic regions, with special attention to performance where infection intensity or prevalence was low.
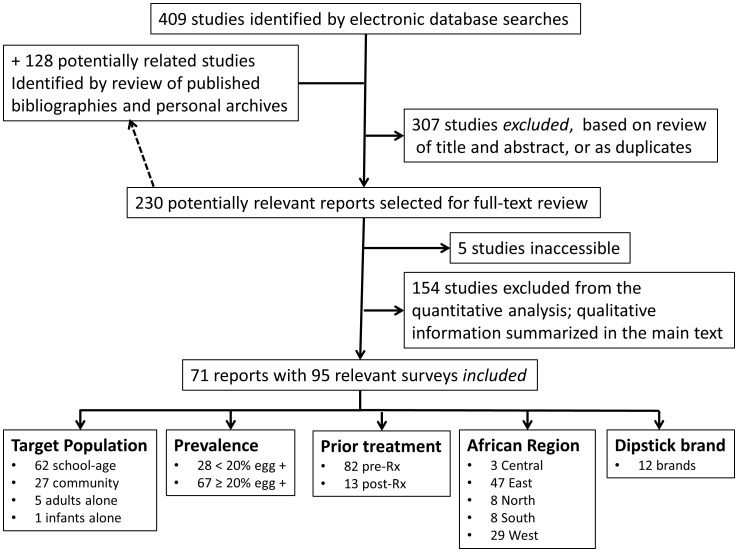
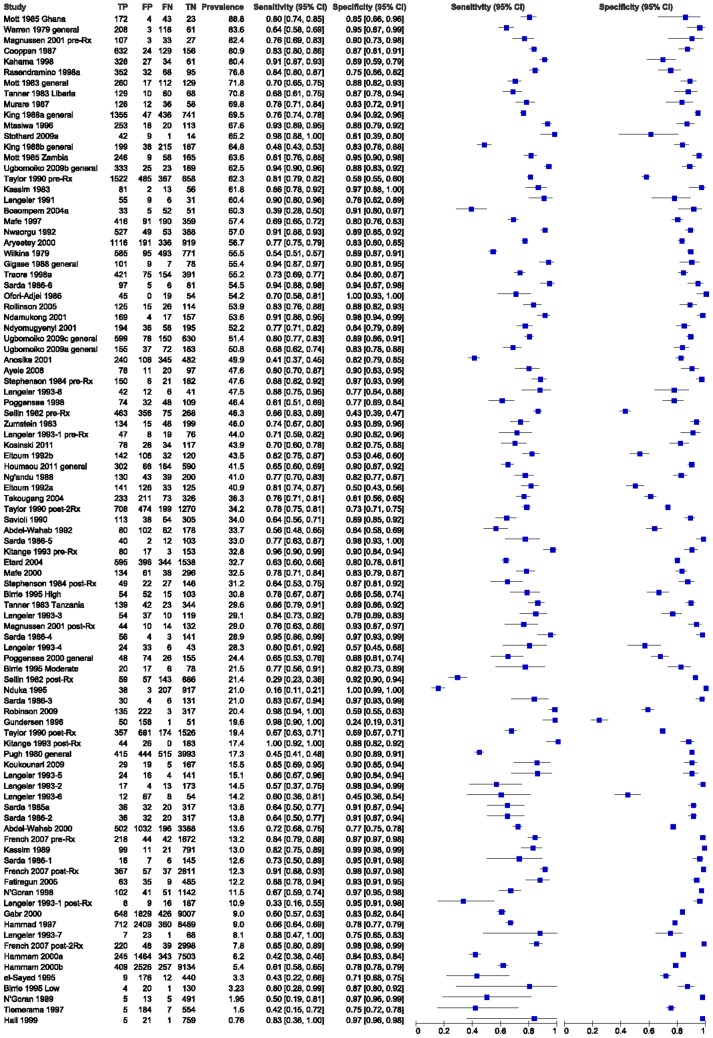
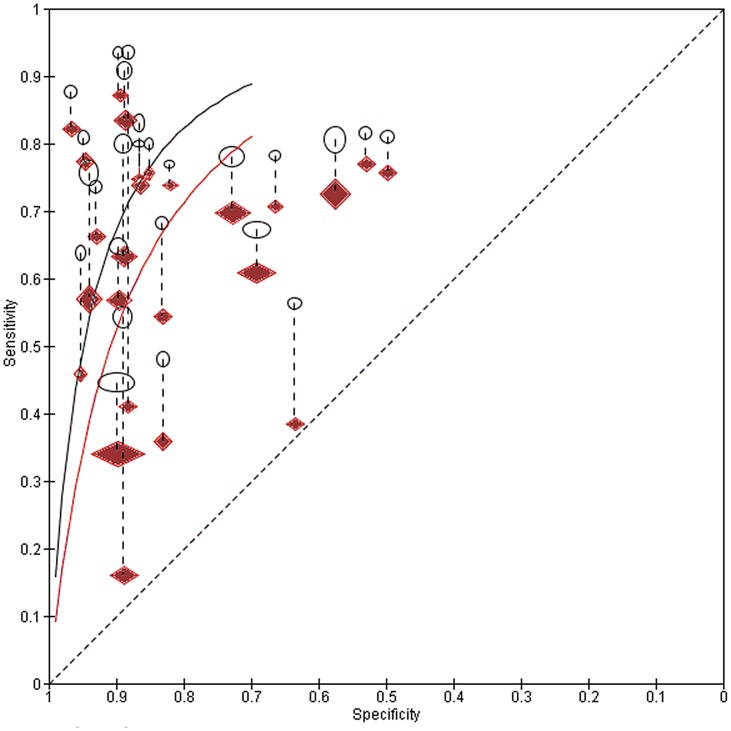
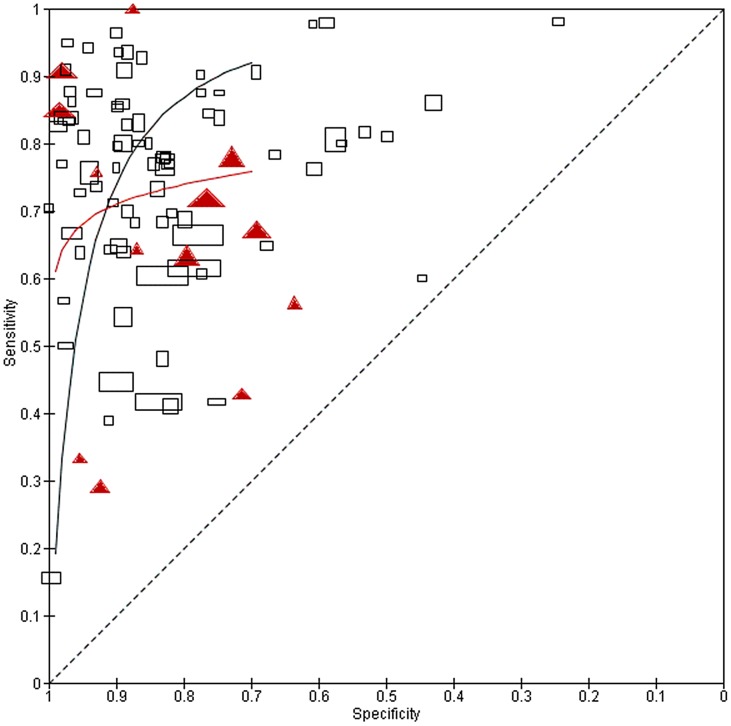
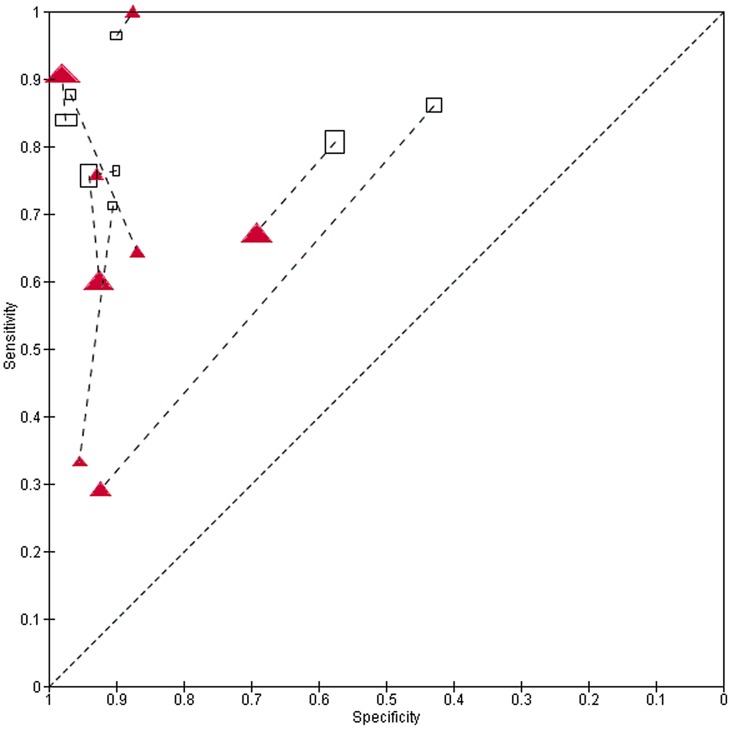
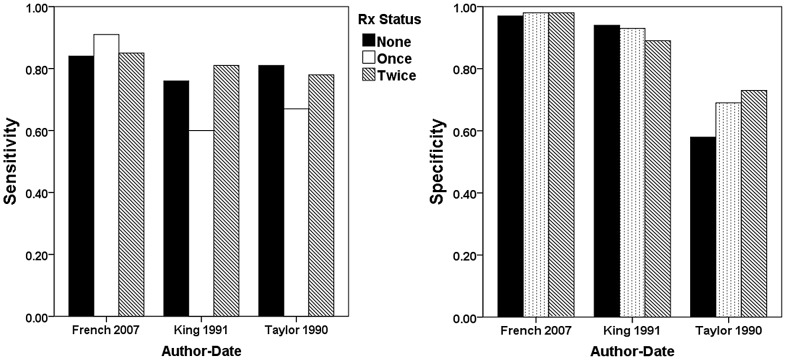
Methodology/principal findings: This review was registered at inception with PROSPERO (CRD42012002165). Included studies were identified by computerized search of online databases and hand search of bibliographies and existing study archives. Eligible studies included published or unpublished population surveys irrespective of date, location, or language that compared dipstick diagnosis of S. haematobium infection to standard egg-count parasitology. For 95 included surveys, variation in dipstick sensitivity and specificity were evaluated according to study size, age- and sex-specific participation, region, local prevalence, treatment status, and other factors potentially affecting test performance. Independent of prevalence, accuracy was greater in surveys of school-age children (vs. adults), whereas performance was less good in North Africa, as compared to other regions. By hierarchical ROC analysis, overall dipstick sensitivity and specificity for detection of egg-positive urine were estimated at 81% and 89%, respectively. Sensitivity was lower among treated populations (72%) and in population subgroups having lower intensity infection (65%). When the insensitivity of egg count testing was considered (and diagnosis inferred instead from combined hematuria and egg-count findings), overall dipstick sensitivity/specificity were 82%/97%, with significantly better sensitivity (92%) in high prevalence settings.
Conclusions/significance: This analysis suggests that dipsticks will continue to serve as very useful adjuncts for monitoring community prevalence following implementation of population-based control of urogenital schistosomiasis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Steinmann P, Keiser J, Bos R, Tanner M, Utzinger J (2006) Schistosomiasis and water resources development: systematic review, meta-analysis, and estimates of people at risk. Lancet Infect Dis 6: 411–425. - PubMed
-
- WHO (2002) Prevention and control of schistosomiasis and soil-transmitted helminthiasis: report of a WHO expert committee. Technical Report Series 912. Geneva: World Health Organization. 912 912. 1–57 p. - PubMed
-
- Schur N, Hurlimann E, Stensgaard AS, Chimfwembe K, Mushinge G, et al. (2011) Spatially explicit Schistosoma infection risk in eastern Africa using Bayesian geostatistical modelling. Acta Trop E-pub ahead of print. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
