

Utility of the mini-cog for detection of cognitive impairment in primary care: data from two spanish studies
- PMID: 24069544
- PMCID: PMC3771448
- DOI: 10.1155/2013/285462
Utility of the mini-cog for detection of cognitive impairment in primary care: data from two spanish studies
Abstract
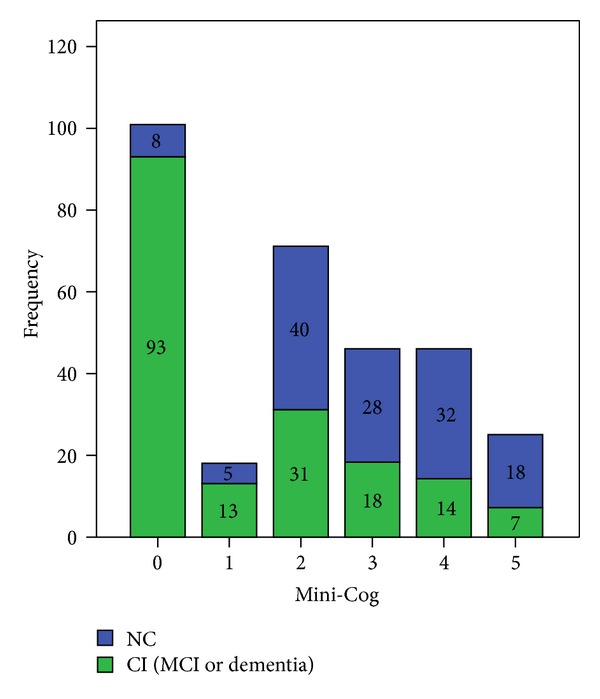
Objectives. To study the utility of the Mini-Cog test for detection of patients with cognitive impairment (CI) in primary care (PC). Methods. We pooled data from two phase III studies conducted in Spain. Patients with complaints or suspicion of CI were consecutively recruited by PC physicians. The cognitive diagnosis was performed by an expert neurologist, after formal neuropsychological evaluation. The Mini-Cog score was calculated post hoc, and its diagnostic utility was evaluated and compared with the utility of the Mini-Mental State (MMS), the Clock Drawing Test (CDT), and the sum of the MMS and the CDT (MMS + CDT) using the area under the receiver operating characteristic curve (AUC). The best cut points were obtained on the basis of diagnostic accuracy (DA) and kappa index. Results. A total sample of 307 subjects (176 CI) was analyzed. The Mini-Cog displayed an AUC (±SE) of 0.78 ± 0.02, which was significantly inferior to the AUC of the CDT (0.84 ± 0.02), the MMS (0.84 ± 0.02), and the MMS + CDT (0.86 ± 0.02). The best cut point of the Mini-Cog was 1/2 (sensitivity 0.60, specificity 0.90, DA 0.73, and kappa index 0.48 ± 0.05). Conclusions. The utility of the Mini-Cog for detection of CI in PC was very modest, clearly inferior to the MMS or the CDT. These results do not permit recommendation of the Mini-Cog in PC.
Figures

References
-
- Luck T, Luppa M, Briel S, Riedel-Heller SG. Incidence of mild cognitive impairment: a systematic review. Dementia and Geriatric Cognitive Disorders. 2010;29(2):164–175. - PubMed
-
- Mitchell AJ, Shiri-Feshki M. Rate of progression of mild cognitive impairment to dementia—meta-analysis of 41 robust inception cohort studies. Acta Psychiatrica Scandinavica. 2009;119(4):252–265. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
