

Lessons from history: morbidity of cold injury in the Royal Marines during the Falklands Conflict of 1982
- PMID: 24070118
- PMCID: PMC3750324
- DOI: 10.1186/2046-7648-2-23
Lessons from history: morbidity of cold injury in the Royal Marines during the Falklands Conflict of 1982
Abstract
Background: Environmental conditions in the Falklands Conflict of 1982 favoured the genesis of cold injuries. Immediately, post-war, cold injury morbidity and its contributory factors were assessed, in the personnel of UK 3 Commando Brigade (3 Cdo Bde).
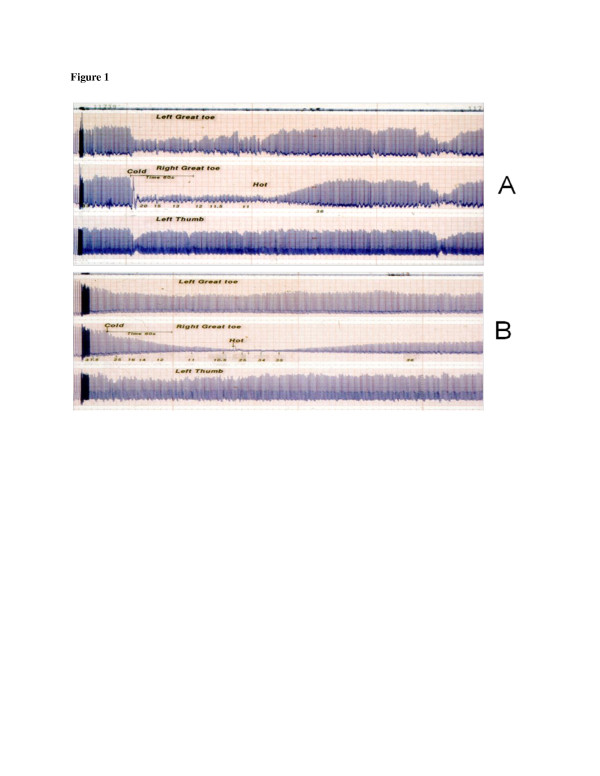
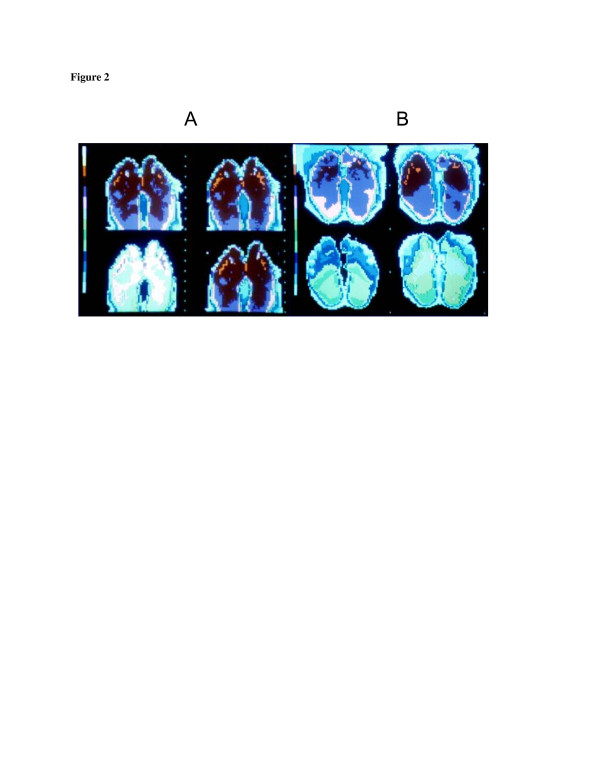
Methods: A questionnaire survey of the 3,006 members of 3 Cdo Bde who landed on the islands was conducted within 6-10 weeks of the end of hostilities. Questions included those relating to features of cold injury, body morphology, age, symptoms experienced, past medical history and other possible contributory causes. Additionally, the unit medical team conducted a cursory examination. Data were sent to the Royal Navy Institute of Naval Medicine (INM), where the degree of likely cold injury was broadly classified ('asymptomatic' 'mild', 'moderate' or 'severe'). A sample (total 109) was then selected at random from each category and subsequently examined and tested at the INM (nerve conduction, photoplethysmography and thermography testing). Forty-seven non-cold exposed sailors acted as a control group. These contemporaneous records have now been identified and interrogated.
Results: Some 2,354 (78%) completed questionnaires were returned, revealing that 1,505 (64%) had experienced symptoms of non-freezing cold injury. The morbidity in the infantry units was significantly greater than that in the support troops (1,051 (76%) vs 454 (46%), p < 0.05). No evidence was found to support an influence of a number of factors, commonly believed to have an aetiological role in the production of cold injury. Whilst there was no significant relationship between past history and cold injury morbidity in the brigade as a whole, or within the infantry units alone, an association was identified in the collective infantry units (73%) and the support/headquarter units (59%) (p < 0.05).In comparison with uninjured sailors who acted as controls (n = 47), nerve conduction was impaired in 35% of those screened some months after returning to the UK, while the photoplethysmography and thermographic responses to a cold sensitivity test showed that most (including those classed by questionnaire as asymptomatic) had residual 'cold sensitivity'.
Conclusions: Although the passage of time has made retrospective interrogation of historical documents hard, the available data do appear to offer valuable historical and clinical insights. Cold injury affected the majority of those fighting in the cold temperate climate of the Falklands. The overwhelming environmental conditions meant that, for most, a past history of cold injury did not appear to represent a risk factor for subsequent injury, as is the case for less severe conditions. Importantly, even asymptomatic individuals when tested often showed physiological evidence of cold injury-perhaps predisposing them to subsequent elevation in risk.
Figures
References
-
- Smith JL, Ritchie J, Dawson J. On the pathology of trench frostbite. Lancet. 1915;186:595–598.
-
- Whayne TF, DeBakey M. Cold Injury, Ground Type. Washington DC: Office of the Surgeon General, Department of the Army; 1958. 48:83–142.
-
- Corbett DO, Benson P. In: Textbook of Military Medicine: Medical Aspects of Harsh Environments. Volume 2. 2. Pandolf AB, Burr RE, editor. Washington DC: Office of the Surgeon General; 2001. Medical aspects of harsh environments: cold-induced injury.
-
- Thompson J. 3 Commando Brigade in the Falklands: No Picnic. Yorkshire: Pen and Sword Books; 1985.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
