

Comorbidity burden and perioperative complications for living kidney donors in the United States
- PMID: 24071651
- PMCID: PMC3789355
- DOI: 10.2215/CJN.12311212
Comorbidity burden and perioperative complications for living kidney donors in the United States
Abstract
Background and objectives: Since 1998, 35% of kidney transplants in the United States have been derived from living donors. Research suggests minimal long-term health consequences after donation, but comprehensive studies are limited. The primary objective was to evaluate trends in comorbidity burden and complications among living donors.
Design, setting, participants, & measurements: The National Inpatient Sample (NIS) was used to identify donors from 1998 to 2010 (n=69,117). Comorbid conditions, complications, and length of stay during hospitalization were evaluated. Outcomes among cohorts undergoing appendectomies, cholecystectomies and nephrectomy for nonmetastatic carcinoma were compared, and sample characteristics were validated with the Scientific Registry of Transplant Recipients (SRTR). Survey regression models were used to identify risk factors for outcomes.
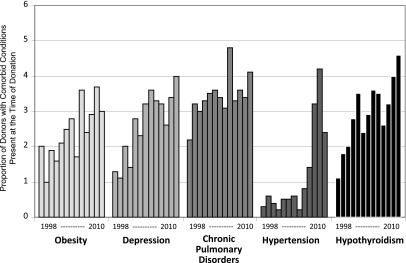
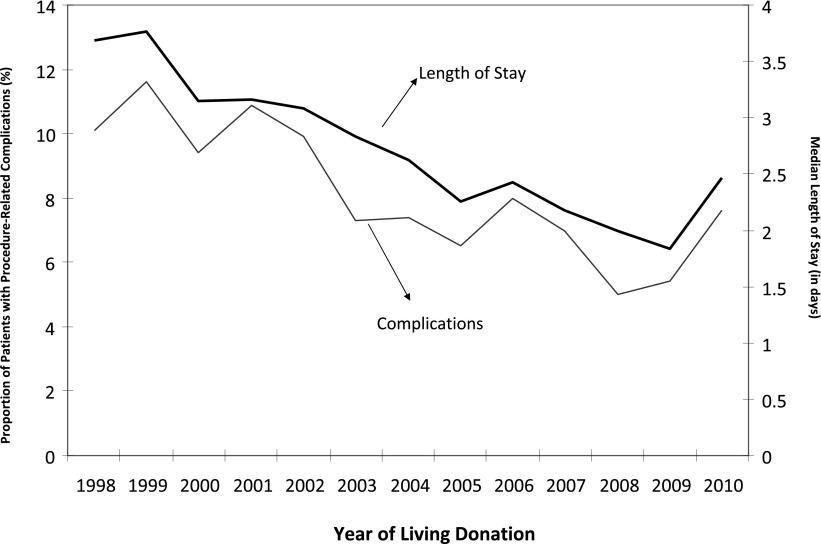
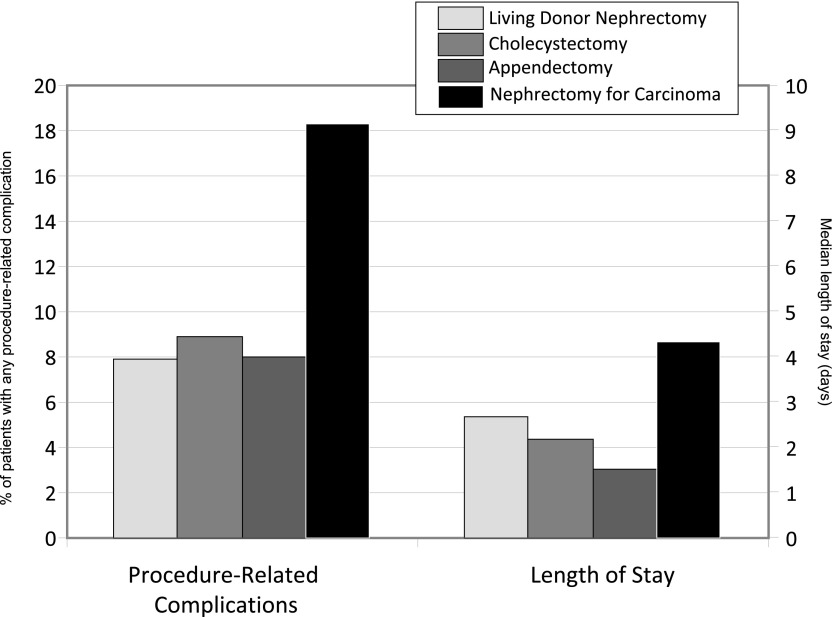
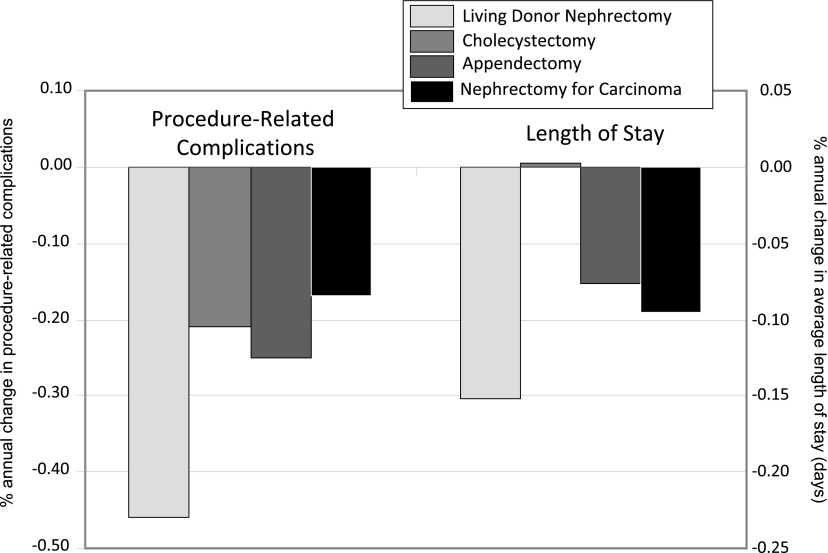
Results: The NIS captured 89% (69,117 of 77,702) of living donors in the United States. Donor characteristics were relatively concordant with those noted in SRTR (mean age, 40.1 versus 40.3 years [P=0.18]; female donors, 59.0% versus 59.1% [P=0.13]; white donors, 68.4% versus 69.8% [P<0.001] for NIS versus SRTR). Incidence of perioperative complications was 7.9% and decreased from 1998 to 2010 (from 10.1% to 7.6%). Men (adjusted odds ratio [AOR], 1.37; 95% confidence interval [CI], 1.20 to 1.56) and donors with hypertension (AOR, 3.35; 95% CI, 2.24 to 5.01) were more likely to have perioperative complications. Median length of stay declined over time (from 3.7 days to 2.5 days), with longer length of stay associated with obesity, depression, hypertension, and pulmonary disorders. Presence of depression (AOR, 1.08; 95% CI, 1.04 to 1.12), hypothyroidism (AOR, 1.07; 95% CI, 1.04 to 1.11), hypertension (AOR, 1.38; 95% CI, 1.27 to 1.49), and obesity (AOR, 1.07; 95% CI, 1.03 to 1.11) increased over time. Complication rates and length of stay were similar for patients undergoing appendectomies and cholecystectomies but were less than those with nephrectomies for carcinoma.
Conclusions: The NIS is a representative sample of living donors. Complications and length of stay after donation have declined over time, while presence of documented comorbid conditions has increased. Patients undergoing appendectomy and cholecystectomy have similar outcomes during hospitalization. Monitoring the health of living donors remains critically important.
Figures
Comment in
-
Better understanding live donor risk through big data.Clin J Am Soc Nephrol. 2013 Oct;8(10):1645-7. doi: 10.2215/CJN.08530813. Epub 2013 Sep 26. Clin J Am Soc Nephrol. 2013. PMID: 24071650 Free PMC article. No abstract available.
References
-
- Organ Procurement and Transplantation Network: Donors Recovered in the U.S. by Donor Type. 2012. Available at: http://optn.transplant.hrsa.gov/latestData/rptData.asp Accessed August 14, 2012
-
- Gill JS, Tonelli M, Johnson N, Kiberd B, Landsberg D, Pereira BJ: The impact of waiting time and comorbid conditions on the survival benefit of kidney transplantation. Kidney Int 68: 2345–2351, 2005 - PubMed
-
- Meier-Kriesche HU, Ojo AO, Port FK, Arndorfer JA, Cibrik DM, Kaplan B: Survival improvement among patients with end-stage renal disease: Trends over time for transplant recipients and wait-listed patients. J Am Soc Nephrol 12: 1293–1296, 2001 - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
