

Impact of hospital teaching status on length of stay and mortality among patients undergoing complex hepatopancreaticobiliary surgery in the USA
- PMID: 24072683
- PMCID: PMC3980573
- DOI: 10.1007/s11605-013-2349-4
Impact of hospital teaching status on length of stay and mortality among patients undergoing complex hepatopancreaticobiliary surgery in the USA
Abstract
Objective: To define the impact of hospital teaching status on length of stay and mortality for patients undergoing complex hepatopancreaticobiliary (HPB) surgery in the USA.
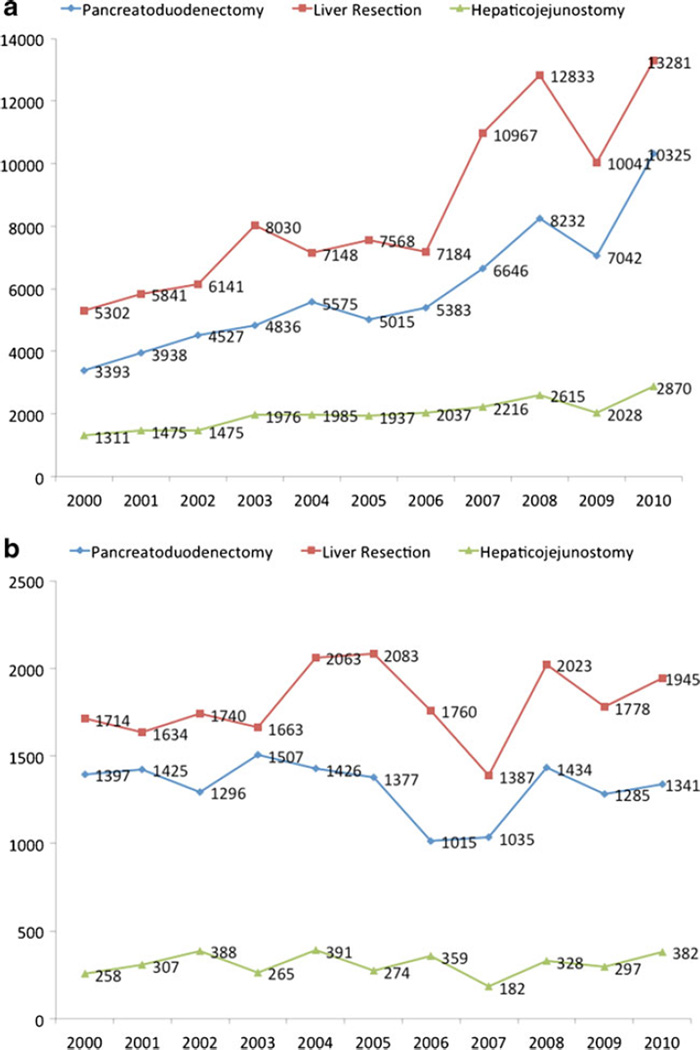
Methods: Using the Nationwide Inpatient Sample, we identified 285,442 patient records that involved a liver resection, pancreatoduodenectomy, other pancreatic resection, or hepaticojejunostomy between years 2000 and 2010. Year-wise distribution of procedures at teaching and non-teaching hospitals was described. The impact of teaching status on in-hospital mortality for operations performed at hospitals in the top tertile of procedure volume was determined using multivariate logistic regression analysis.
Results: A majority of patients were under 65 years of age (59.6 %), white (74.0 %), admitted on an elective basis (77.3 %), and had a low comorbidity burden (70.5 %). Ninety percent were operated upon at hospitals in the top tertile of yearly procedure volume. Among patients undergoing an operation at a hospital in the top tertile of procedure volume (>25/year), non-teaching status was associated with an increased risk of in-hospital death (OR 1.47 [1.3, 1.7]). Other factors associated with increased risk of mortality were older patient age (OR 2.52 [2.3, 2.8]), male gender (OR 1.73 [1.6, 1.9]), higher comorbidity burden (OR 1.49 [1.3, 1.7]), non-elective admission (OR 3.32 [2.9, 4.0]), and having a complication during in-hospital stay (OR 2.53 [2.2, 3.0]), while individuals with private insurance had a lower risk of in-hospital mortality (OR 0.45 [0.4, 0.5]). After controlling for other covariates, undergoing complex HPB surgery at a non-teaching hospital remained independently associated with 32 % increased odds of death as (OR 1.32, 95 % CI 1.11-1.58; P < 0.001).
Conclusions: Even among high-volume hospitals, patients undergoing complex HPB have better outcomes at teaching vs. non-teaching hospitals. While procedural volume is an established factor associated with surgical outcomes among patients undergoing complex HPB procedures, other hospital-level factors such as teaching status have an important impact on peri-operative outcomes.
Figures
References
-
- Association of American Medical Colleges; 2010. Data on teaching hospitals and charity care.
-
- Sorra J, et al. Rockville, MD: Agency for Healthcare Research and Quality; 2012. Hospital Survey on Patient Safety Culture: 2012 User Comparative Database Report.
-
- Stewart DB, et al. Rectal Cancer and Teaching Hospitals: Hospital Teaching Status Affects Use of Neoadjuvant Radiation and Survival for Rectal Cancer Patients. Annals of Surgical Oncology. 2013;20(4):1156–1163. - PubMed
-
- Grosskopf S, Margaritis D, Valdmanis V. Comparing teaching and non-teaching hospitals: a frontier approach (teaching vs. nonteaching hospitals) Health Care Manag Sci. 2001;4(2):83–90. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
