

Polycystic ovary syndrome: effect and mechanisms of acupuncture for ovulation induction
- PMID: 24073009
- PMCID: PMC3773899
- DOI: 10.1155/2013/762615
Polycystic ovary syndrome: effect and mechanisms of acupuncture for ovulation induction
Abstract
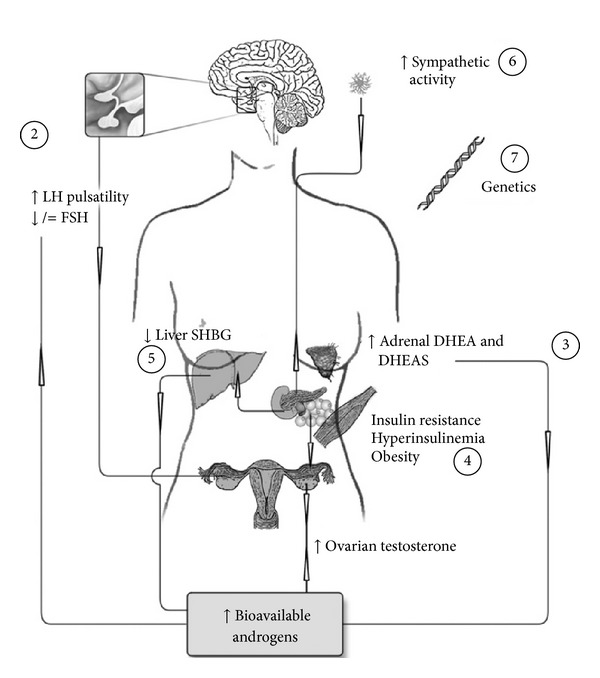
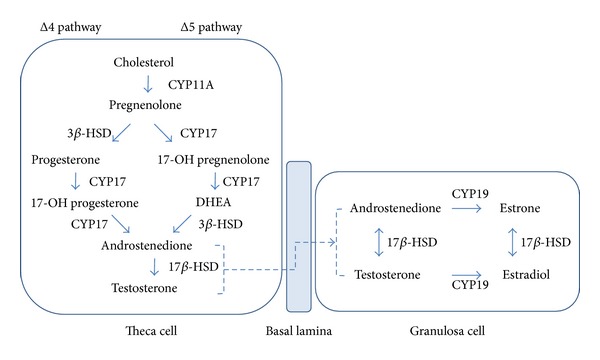
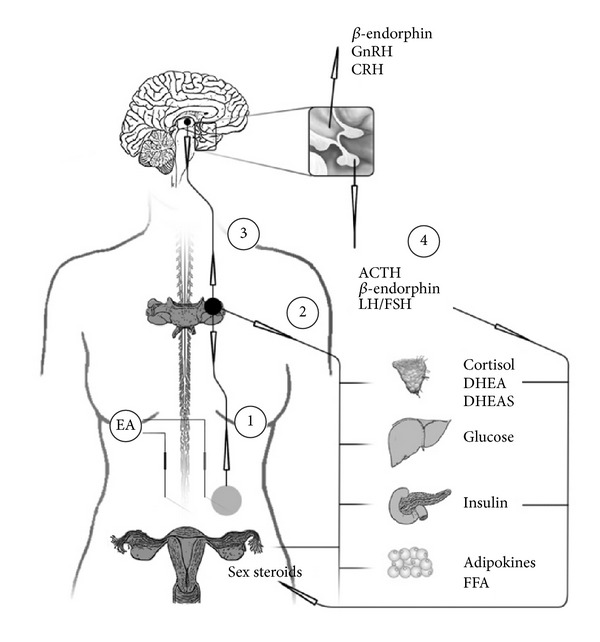
Polycystic ovary syndrome (PCOS), the most common endocrine disorder among women of reproductive age, is characterized by the coexistence of hyperandrogenism, ovulatory dysfunction, and polycystic ovaries (PCO). PCOS also represents the largest part of female oligoovulatory infertility, and the management of ovulatory and menstrual dysfunction, comprises a third of the high costs of PCOS treatment. Current pharmacological and surgical treatments for reproductive symptoms are effective, however, associated with negative side effects, such as cardiovascular complications and multiple pregnancies. For menstrual irregularities and ovulation induction in women with PCOS, acupuncture has indicated beneficial effects. This review will focus on the results from randomized controlled acupuncture trials for regulation of menstrual dysfunction and for inducing ovulation in women with PCOS although there are uncontrolled trials with nonetheless interesting results. Animal experimental studies will be further discussed when they can provide a more mechanistic explanatory view.
Figures
References
-
- Yildiz BO, Bozdag G, Yapici Z, Esinler I, Yarali H. Prevalence, phenotype and cardiometabolic risk of polycystic ovary syndrome under different diagnostic criteria. Human Reproduction. 2012;27:3067–3073. - PubMed
-
- March WA, Moore VM, Willson KJ, Phillips DIW, Norman RJ, Davies MJ. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Human Reproduction. 2010;25(2):544–551. - PubMed
-
- Wild RA, Carmina E, Diamanti-Kandarakis E, et al. Assessment of cardiovascular risk and prevention of cardiovascular disease in women with the polycystic ovary syndrome: a consensus statement by the androgen excess and polycystic ovary syndrome (AE-PCOS) society. The Journal of Clinical Endocrinology and Metabolism. 2010;95(5):2038–2049. - PubMed
-
- Sathyapalan T, Atkin SL. Recent advances in cardiovascular aspects of polycystic ovary syndrome. European Journal of Endocrinology. 2012;166(4):575–583. - PubMed
-
- (NIH) NIoH. Evidence-Based Methodology Workshop on Polycystic Ovary Syndrome. 2012.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
