

Instrument-assisted cross fiber massage increases tissue perfusion and alters microvascular morphology in the vicinity of healing knee ligaments
- PMID: 24073942
- PMCID: PMC3852802
- DOI: 10.1186/1472-6882-13-240
Instrument-assisted cross fiber massage increases tissue perfusion and alters microvascular morphology in the vicinity of healing knee ligaments
Abstract
Background: Ligament injuries are common clinical problems for which there are few established interventions. Instrument-assisted cross fiber massage (IACFM) was recently shown to accelerate the restoration of biomechanical properties in injured rodent knee medial collateral ligaments (MCL). The current study aimed to investigate the influence of IACFM on regional perfusion and vascularity in the vicinity of healing rodent knee MCL injuries.
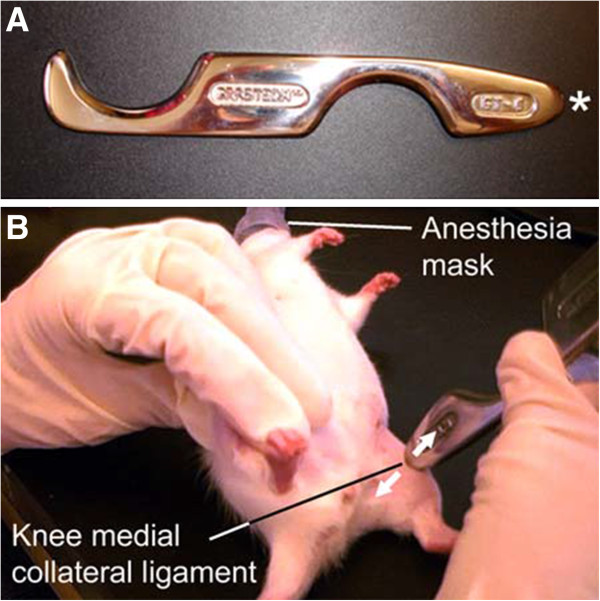
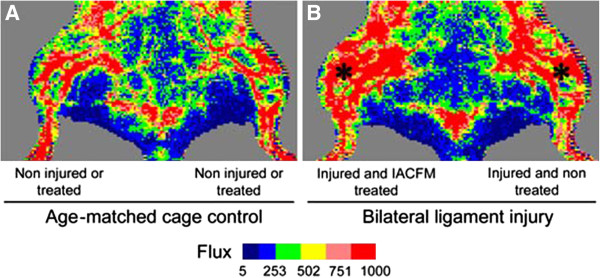
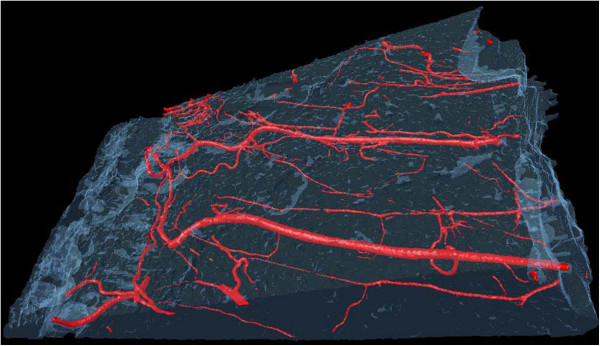
Methods: Bilateral knee MCL injuries were induced in female Sprague-Dawley rats. Commencing 1 week post-injury, 1 minute of IACFM was introduced unilaterally 3 times/week for 3 weeks. The contralateral injured MCL served as an internal control. Regional tissue perfusion was assessed in vivo throughout healing using laser Doppler imaging, whereas regional microvascular morphology was assessed ex vivo via micro-computed tomography of vessels filled with contrast.
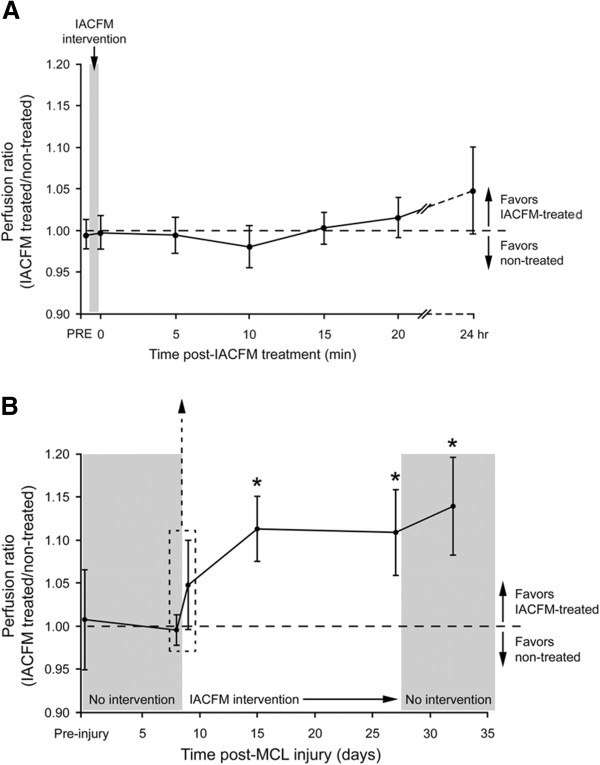
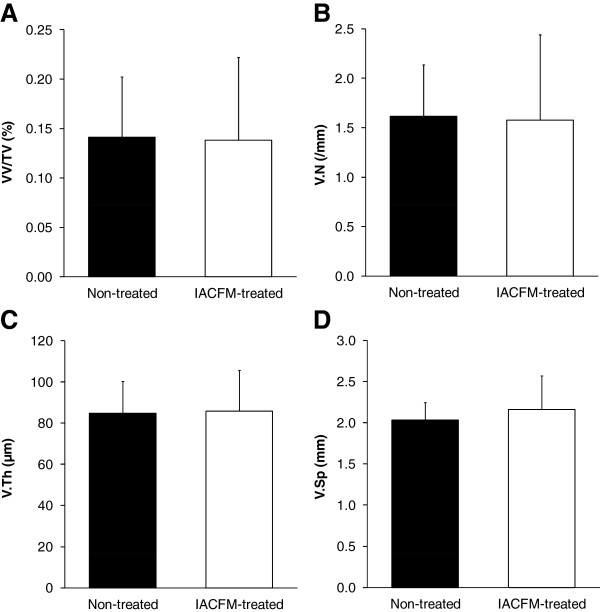
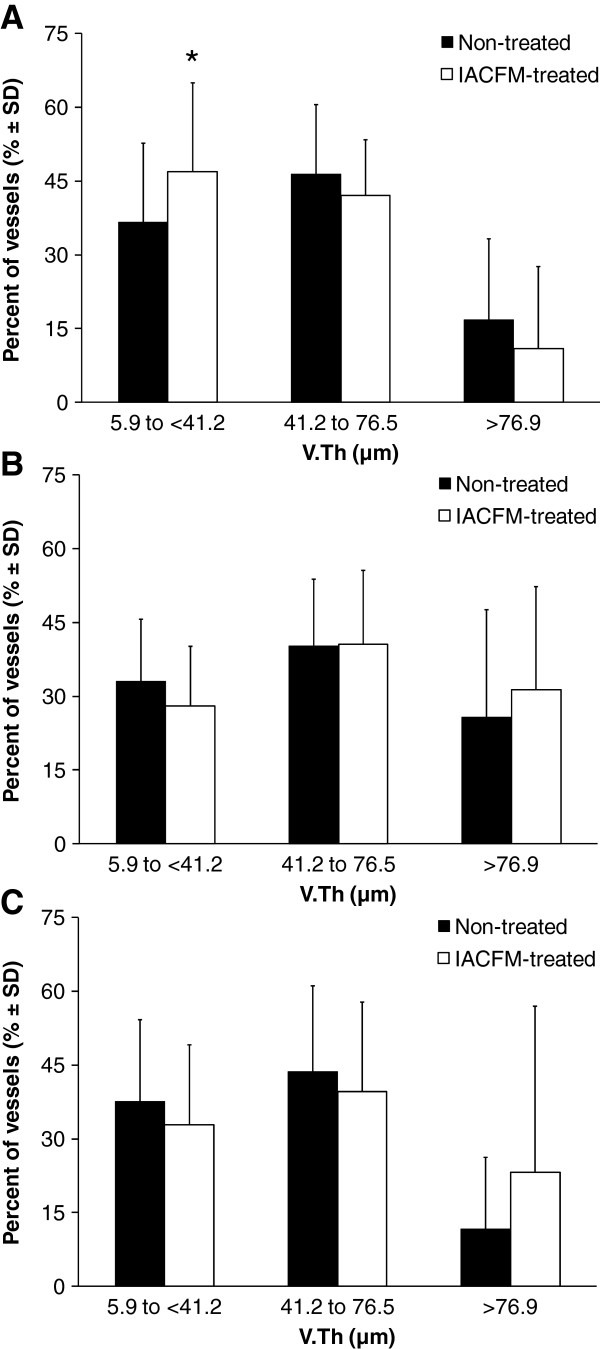
Results: IACFM had no effect on tissue perfusion when assessed immediately, or at 5, 10, 15 or 20 min following intervention (all p > 0.05). However, IACFM-treated hindlimbs had enhanced tissue perfusion when assessed 1 day following the 4th and 9th (last) treatment sessions (all p < 0.05). IACFM-treated hindlimbs also had greater perfusion when assessed 1 wk following the final treatment session (32 days post-injury) (p < 0.05). Subsequent investigation of microvascular morphology found IACFM to increase the proportion of arteriole-sized blood vessels (5.9 to <41.2 μm) in the tibial third of the ligament (p < 0.05).
Conclusions: These findings suggest IACFM alters regional perfusion and vascularity in the vicinity of healing rodent knee MCL injuries. This effect may contribute to the beneficial effect of IACFM observed on the recovery of knee ligament biomechanical properties following injury.
Figures
References
-
- Fernandez WG, Yard EE, Comstock RD. Epidemiology of lower extremity injuries among U.S. high school athletes. Acad Emerg Med. 2007;14(7):641–645. - PubMed
-
- Tyler TF, McHugh MP, Mirabella MR, Mullaney MJ, Nicholas SJ. Risk factors for noncontact ankle sprains in high school football players: the role of previous ankle sprains and body mass index. Am J Sports Med. 2006;34(3):471–475. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
