

Clinical testing of otolith function: perceptual thresholds and myogenic potentials
- PMID: 24077672
- PMCID: PMC3825026
- DOI: 10.1007/s10162-013-0416-x
Clinical testing of otolith function: perceptual thresholds and myogenic potentials
Abstract
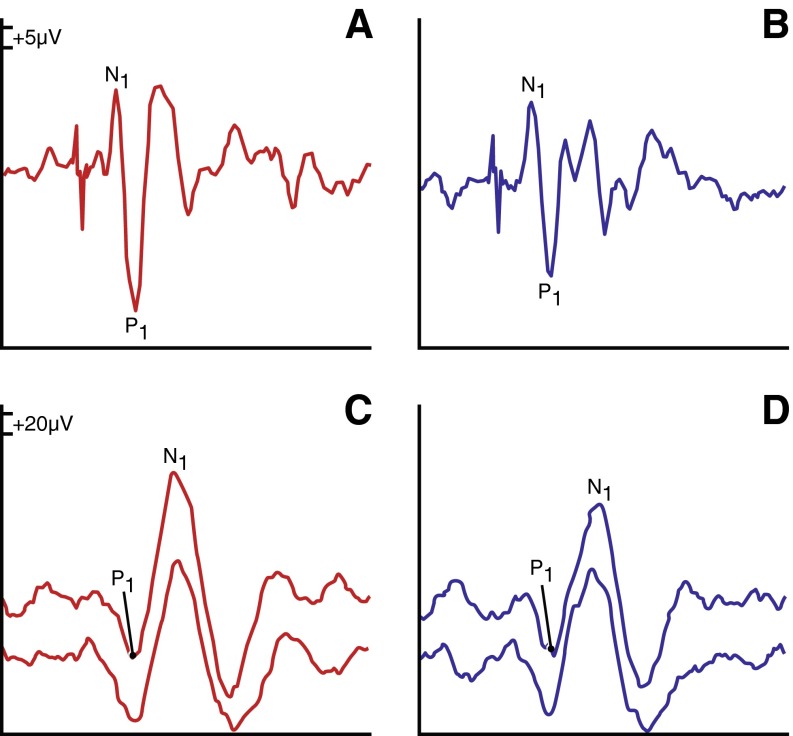
Cervical and ocular vestibular-evoked myogenic potential (cVEMP/oVEMP) tests are widely used clinical tests of otolith function. However, VEMP testing may not be the ideal measure of otolith function given the significant inter-individual variability in responses and given that the stimuli used to elicit VEMPs are not physiological. We therefore evaluated linear motion perceptual threshold testing compared with cVEMP and oVEMP testing as measures of saccular and utricular function, respectively. A multi-axis motion platform was used to measure horizontal (along the inter-aural and naso-occipital axes) and vertical motion perceptual thresholds. These findings were compared with the vibration-evoked oVEMP as a measure of utricular function and sound-evoked cVEMP as a measure of saccular function. We also considered how perceptual threshold and cVEMP/oVEMP testing are each associated with Dizziness Handicap Inventory (DHI) scores. We enrolled 33 patients with bilateral vestibulopathy of different severities and 42 controls to have sufficient variability in otolith function. Subjects with abnormal oVEMP amplitudes had significantly higher (poorer) perceptual thresholds in the inter-aural and naso-occipital axes in age-adjusted analyses; no significant associations were observed for vertical perceptual thresholds and cVEMP amplitudes. Both oVEMP amplitudes and naso-occipital axis perceptual thresholds were significantly associated with DHI scores. These data suggest that horizontal perceptual thresholds and oVEMPs may estimate the same underlying physiological construct: utricular function.
Figures


Similar articles
-
Comparison of linear motion perception thresholds in vestibular migraine and Menière's disease.Eur Arch Otorhinolaryngol. 2016 Oct;273(10):2931-9. doi: 10.1007/s00405-015-3835-y. Epub 2016 Jan 4. Eur Arch Otorhinolaryngol. 2016. PMID: 26728484 Free PMC article.
-
Effects of cochlear implants on otolith function as evaluated by vestibulo-ocular reflex and vestibular evoked myogenic potentials.Auris Nasus Larynx. 2019 Dec;46(6):836-843. doi: 10.1016/j.anl.2019.03.011. Epub 2019 Apr 19. Auris Nasus Larynx. 2019. PMID: 31010711
-
Ocular vestibular evoked myogenic potentials to air conduction (AC oVEMP): useful in clinical practice?Otolaryngol Pol. 2011 Sep-Oct;65(5):333-8. doi: 10.1016/S0030-6657(11)70722-3. Otolaryngol Pol. 2011. PMID: 22078282 Review.
-
The influence of unilateral saccular impairment on functional balance performance and self-report dizziness.J Am Acad Audiol. 2011 Sep;22(8):542-9; quiz 560-1. doi: 10.3766/jaaa.22.8.6. J Am Acad Audiol. 2011. PMID: 22031678
-
Otolith Function Testing.Adv Otorhinolaryngol. 2019;82:47-55. doi: 10.1159/000490271. Epub 2019 Jan 15. Adv Otorhinolaryngol. 2019. PMID: 30947185 Review.
Cited by
-
Vestibular Thresholds: A Review of Advances and Challenges in Clinical Applications.Front Neurol. 2021 Feb 19;12:643634. doi: 10.3389/fneur.2021.643634. eCollection 2021. Front Neurol. 2021. PMID: 33679594 Free PMC article. Review.
-
Recruitment properties and significance of short latency reflexes in neck and eye muscles evoked by brief lateral head accelerations.Exp Brain Res. 2014 Sep;232(9):2977-88. doi: 10.1007/s00221-014-3980-3. Epub 2014 May 18. Exp Brain Res. 2014. PMID: 24838556 Free PMC article.
-
Impact of gravity on the perception of linear motion.J Neurophysiol. 2021 Sep 1;126(3):875-887. doi: 10.1152/jn.00274.2021. Epub 2021 Jul 28. J Neurophysiol. 2021. PMID: 34320866 Free PMC article.
-
Absence of Rotation Perception during Warm Water Caloric Irrigation in Some Seniors with Postural Instability.Front Neurol. 2016 Jan 25;7:4. doi: 10.3389/fneur.2016.00004. eCollection 2016. Front Neurol. 2016. PMID: 26834699 Free PMC article.
-
Vestibular therapy to reduce falls in people with Alzheimer's disease: study protocol for a pilot randomized controlled trial.Pilot Feasibility Stud. 2022 Aug 2;8(1):167. doi: 10.1186/s40814-022-01133-w. Pilot Feasibility Stud. 2022. PMID: 35918757 Free PMC article.
References
-
- Benson AJ, Spencer MB, et al. Thresholds for the detection of the direction of whole-body, linear movement in the horizontal plane. Aviat Space Environ Med. 1986;57(11):1088–1096. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
