

Parathyroid hormone and parathyroid hormone-related protein analogs as therapies for osteoporosis
- PMID: 24078470
- PMCID: PMC3874264
- DOI: 10.1007/s11914-013-0171-2
Parathyroid hormone and parathyroid hormone-related protein analogs as therapies for osteoporosis
Abstract
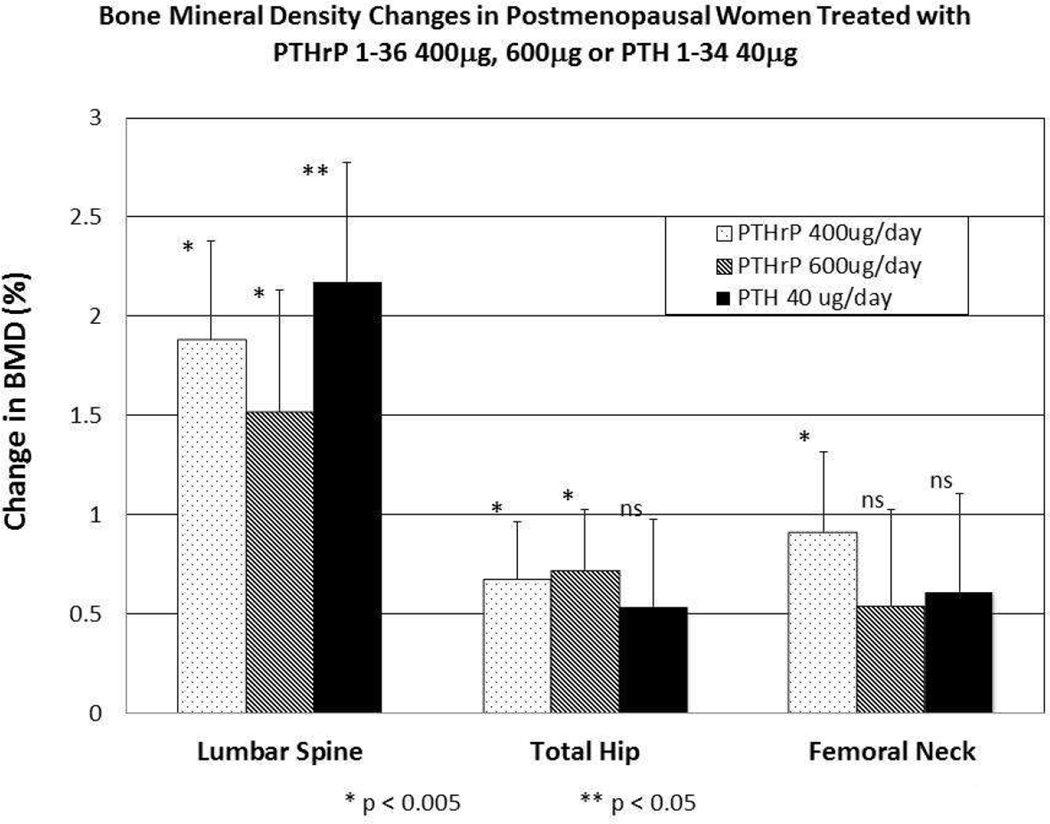
Osteoporotic fractures result in significant morbidity and mortality. Anabolic agents reverse the negative skeletal balance that characterizes osteoporosis by stimulating osteoblast-dependent bone formation to a greater degree than osteoclast-dependent bone resorption. Parathyroid hormone (PTH) and parathyroid hormone- related protein (PTHrP) are peptide hormones, which have anabolic actions when administered intermittently. The only FDA-approved anabolic bone agent for the treatment of osteoporosis in the United States is PTH 1-34, or teriparatide, administered by daily subcutaneous injections. However, PTH 1-84 is also available in Europe. Synthetic human PTHrP 1-36 and a PTHrP 1-34 analog, BA058, have also been shown to increase lumbar spine bone density. These agents and several other PTH and PTHrP analogs, including some which are not administered as injections, continue to be investigated as potential anabolic therapies for osteoporosis.
Conflict of interest statement
M Augustine works for an institution that has received an NIH grant.
MJ Horwitz works for an institution that has received an NIH grant, is an NPS consultant, and has received royalties as a chapter author for Up To Date.
Figures
References
-
- Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785–795. - PubMed
-
- [Accessed May 2013];WHO Scientific Group on the Assessment of Osteoporosis at Primary Health Care Level. Available at http://www.who.int/chp/topics/Osteoporosis.pdf.
-
- Dempster DW, Zhou H, Recker RR, et al. Skeletal histomorphometry in subjects on teriparatide or zoledronic acid therapy (SHOTZ) study: a randomized controlled trial. J Clin Endocrinol Metab. 2012;97:2799–2808. - PubMed
-
- Watts NB, Harris ST, Genant HK, et al. Intermittent cyclical etidronate treatment of postmenopausal osteoporosis. N Engl J Med. 1990;323:73–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
