

A qualitative study of patients' perceptions and priorities when living with primary frozen shoulder
- PMID: 24078753
- PMCID: PMC3787409
- DOI: 10.1136/bmjopen-2013-003452
A qualitative study of patients' perceptions and priorities when living with primary frozen shoulder
Abstract
Objectives: To elucidate the experiences and perceptions of people living with primary frozen shoulder and their priorities for treatment.
Design: Qualitative study design using semistructured interviews.
Setting: General practitioner (GP) and musculoskeletal clinics in primary and secondary care in one National Health Service Trust in England.
Participants: 12 patients diagnosed with primary frozen shoulder were purposively recruited from a GP's surgery, community clinics and hospital clinics. Recruitment targeted the phases of frozen shoulder: pain predominant (n=5), stiffness predominant (n=4) and residual stiffness predominant following hospital treatment (n=2). One participant dropped out.
Inclusion criteria: adult, male and female patients of any age, attending the clinics, who had been diagnosed with primary frozen shoulder.
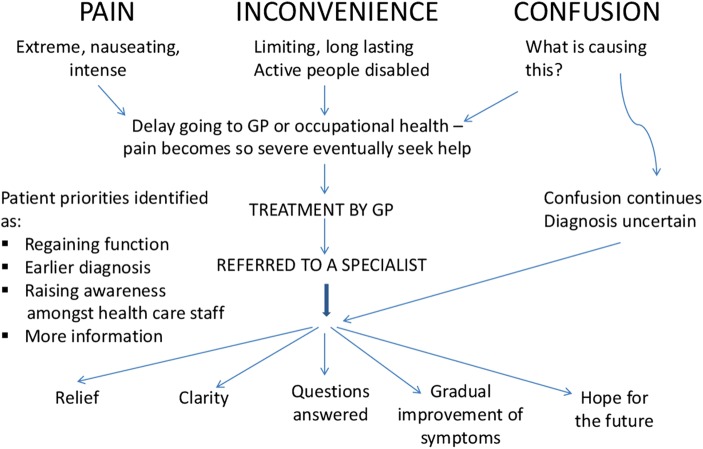
Results: The most important experiential themes identified by participants were: pain which was severe as well as inexplicable; inconvenience/disability arising from increasing restriction of movement (due to pain initially, gradually giving way to stiffness); confusion/anxiety associated with delay in diagnosis and uncertainty about the implications for the future; and treatment-related aspects. Participants not directly referred to a specialist (whether physiotherapist, physician or surgeon) wanted a faster, better-defined care pathway. Specialist consultation brought more definitive diagnosis, relief from anxiety and usually self-rated improvement. The main treatment priority was improved function, though there was recognition that this might be facilitated by relief of pain or stiffness. There was a general lack of information from clinicians about the condition with over-reliance on verbal communication and very little written information.
Conclusions: Awareness of frozen shoulder should be increased among non-specialists and the best available information made accessible for patients. Our results also highlight the importance of patient participation in frozen shoulder research.
Keywords: Pain Management.
References
-
- Hand GCR, Athanasou NA, Matthews T, et al. The pathology of frozen shoulder. J Bone Joint Surg Br 2007;89:928–32 - PubMed
-
- Kelley MJ, McClure PW, Leggin BG. Frozen shoulder: evidence and a proposed model guiding rehabilitation. J Orthop Sports Phys Ther 2009;39:135–48 - PubMed
-
- Robinson CM, Seah KTM, Chee YH, et al. Frozen shoulder. J Bone Joint Surg Br 2012;94:1–9 http://www.ncbi.nlm.nih.gov/pubmed/22219239 - PubMed
-
- Milgrom C, Novack V, Weil Y, et al. Risk factors for idiopathic frozen shoulder. Isr Med Assoc J 2008;10:361–4 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical