

Biliary drainage method and temporal trends in patients admitted with cholangitis: a national audit
- PMID: 24078935
- PMCID: PMC3956005
- DOI: 10.1155/2013/175143
Biliary drainage method and temporal trends in patients admitted with cholangitis: a national audit
Abstract
Background: In patients presenting with ascending cholangitis, better outcomes are reported in those undergoing endoscopic retrograde cholangiopancreatography (ERCP) compared with surgical drainage.
Objective: To identify factors associated with the type of intervention, and to examine temporal trends in the treatment of ascending cholangitis.
Methods: Data were extracted from the Nationwide Inpatient Sample. Patients ≥18 years of age with a diagnosis of cholangitis between 1998 and 2009 were selected. Temporal trends were assessed using Poisson regression models. Multivariable models were fitted to predict the likelihood of a patient undergoing ERCP, percutaneous or surgical drainage, or no drainage.
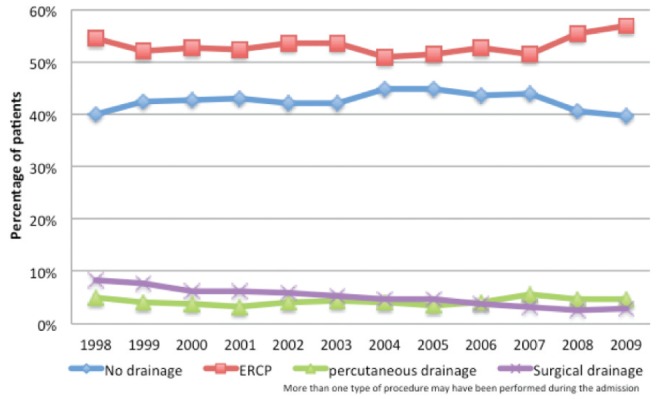
Results: A weighted estimate of 248,942 patients admitted for cholangitis was identified. Overall, 131,052 patients were treated with ERCP (52.6%), 10,486 with percutaneous drainage (4.2%) and 12,460 with surgical drainage (5.0%); 43.0% did not receive drainage during the admission. Temporal trends between 1998 and 2009 showed a decline in surgical and percutaneous drainage, and a rise in ERCP. In multivariable analyses adjusted for clustering, ERCP and percutaneous drainage were more often performed in institutions with a high volume of admissions for cholangitis, those with a greater bed number and hospitals located in urban areas.
Conclusion: Over the past decade, the use of surgical and percutaneous drainage has decreased while that of ERCP has risen. Patients treated at institutions with a low volume of admissions for cholangitis, small bed number and in rural areas were less likely to undergo ERCP or percutaneous drainage.
HISTORIQUE :: Chez les patients présentant une cholangite ascendante, ceux qui subissent une cholangiopancréatographie rétrograde endoscopique (CPRE) s’en sortent mieux que ceux qui subissent un drainage chirurgical.
OBJECTIF :: Déterminer les facteurs associés au type d’intervention et examiner les tendances temporelles dans le traitement de la cholangite ascendante.
MÉTHODOLOGIE :: Les chercheurs ont extrait les données du Nationwide Inpatient Sample. Ils ont sélectionné les patients de 18 ans ou plus dont la cholangite avait été diagnostiquée entre 1998 and 2009. Ils ont évalué les tendances temporelles au moyen des modèles de régression de Poisson. Ils ont corrigé les modèles multivariables pour prédire la probabilité qu’un patient subisse une CPRE ou un drainage percutané ou chirurgical ou qu’il ne subisse pas de drainage.
RÉSULTATS :: Les chercheurs ont recensé une estimation pondérée de 248 942 patients hospitalisés en raison d’une cholangite. Dans l’ensemble, 131 052 patients ont subi une CPRE (52,6 %), 10 486, un drainage percutané (4,2 %) et 12 460, un drainage chirurgical (5,0 %), tandis que 43,0 % n’ont pas subi de drainage pendant leur hospitalisation. Les tendances temporelles entre 1998 et 2009 ont révélé un fléchissement des drainages chirurgicaux et percutanés et une augmentation des CPRE. Selon les analyses multivariables corrigées pour tenir compte des regroupements, la CPRE et le drainage percutané étaient davantage exécutés dans les établissements présentant un fort volume d’hospitalisations en raison d’une cholangite, comptant un plus grand nombre de lits et situés en milieu urbain.
CONCLUSION :: Depuis dix ans, le recours au drainage chirurgical ou percutané a diminué tandis que les CPRE ont augmenté. Les patients étaient moins susceptibles de subir une CPRE ou un drainage percutané s’ils étaient traités dans des établissements situés en région rurale et comptant peu d’hospitalisations en raison d’une cholangite et peu de lits.
Figures
References
-
- Lai EC, Mok FP, Tan ES, et al. Endoscopic biliary drainage for severe acute cholangitis. N Engl J Med. 1992;326:1582–6. - PubMed
-
- United States Census Bureau 2000. [cited 2011] < www.census.gov> (Accessed December 2011).
-
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous