

Etiology and therapeutic approach to elevated lactate levels
- PMID: 24079682
- PMCID: PMC3975915
- DOI: 10.1016/j.mayocp.2013.06.012
Etiology and therapeutic approach to elevated lactate levels
Abstract
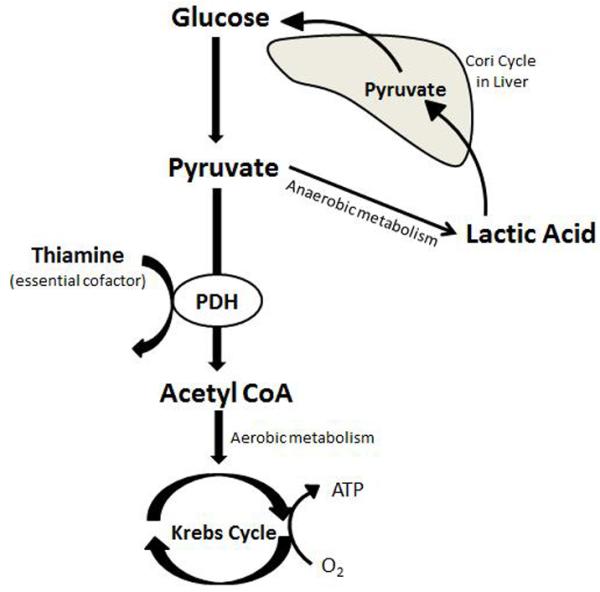
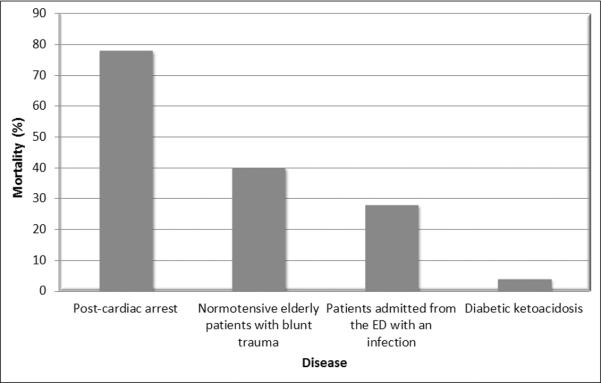
Lactate levels are commonly evaluated in acutely ill patients. Although most often used in the context of evaluating shock, lactate levels can be elevated for many reasons. While tissue hypoperfusion may be the most common cause of elevation, many other etiologies or contributing factors exist. Clinicians need to be aware of the many potential causes of lactate level elevation as the clinical and prognostic importance of an elevated lactate level varies widely by disease state. Moreover, specific therapy may need to be tailored to the underlying cause of elevation. The present review is based on a comprehensive PubMed search between the dates of January 1, 1960, to April 30, 2013, using the search term lactate or lactic acidosis combined with known associations, such as shock, sepsis, cardiac arrest, trauma, seizure, ischemia, diabetic ketoacidosis, thiamine, malignancy, liver, toxins, overdose, and medication. We provide an overview of the pathogenesis of lactate level elevation followed by an in-depth look at the varied etiologies, including medication-related causes. The strengths and weaknesses of lactate as a diagnostic/prognostic tool and its potential use as a clinical end point of resuscitation are discussed. The review ends with some general recommendations on the management of patients with elevated lactate levels.
Keywords: DKA; ScvO(2); central venous oxygen saturation; diabetic ketoacidosis.
Copyright © 2013 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Broder G, Weil MH. Excess Lactate: An Index of Reversibility of Shock in Human Patients. Science. 1964 Mar 27;143:1457–1459. - PubMed
-
- Woods HFC, Robert . Clinical and biochemical aspects of lactic acidosis. Blackwell Scientific; Oxford: 1976.
-
- Consoli A, Nurjhan N, Reilly JJ, Jr., Bier DM, Gerich JE. Contribution of liver and skeletal muscle to alanine and lactate metabolism in humans. The American journal of physiology. 1990 Nov;259(5 Pt 1):E677–684. - PubMed
-
- van Hall G. Lactate kinetics in human tissues at rest and during exercise. Acta Physiol (Oxf) 2010 Aug;199(4):499–508. - PubMed
-
- Connor H, Woods HF, Ledingham JG, Murray JD. A model of L(+)-lactate metabolism in normal man. Annals of nutrition & metabolism. 1982;26(4):254–263. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
