

Repetitive myocardial ischemia promotes coronary growth in the adult mammalian heart
- PMID: 24080909
- PMCID: PMC3835243
- DOI: 10.1161/JAHA.113.000343
Repetitive myocardial ischemia promotes coronary growth in the adult mammalian heart
Abstract
Background: Coronary artery disease and ischemic cardiomyopathy represent the leading cause of heart failure and continue to grow at exponential rates. Despite widespread availability of coronary bypass surgery and percutaneous coronary intervention, subsequent ischemic events and progression to heart failure continue to be common occurrences. Previous studies have shown that a subgroup of patients develop collateral blood vessels that serve to connect patent and occluded arteries and restore perfusion to ischemic territories. The presence of coronary collaterals has been correlated with improved clinical outcomes; however, the molecular mechanisms governing this process remain largely unknown.
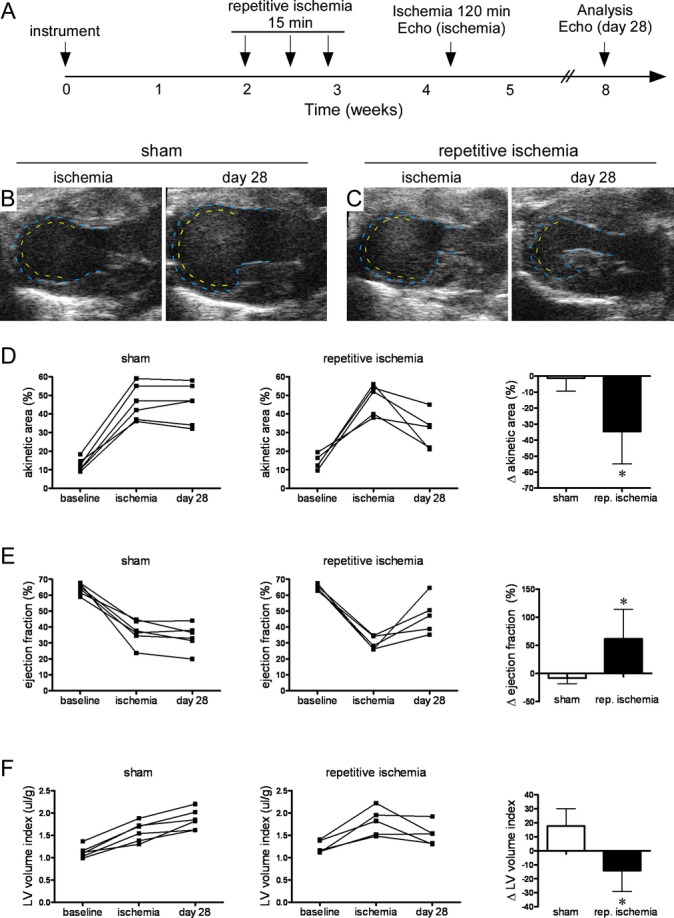
Methods and results: To date, no mouse models of coronary arterial growth have been described. Using a closed-chest model of myocardial ischemia, we have demonstrated that brief episodes of repetitive ischemia are sufficient to promote the growth of both large coronary arteries and the microvasculature. Induction of large coronary artery and microvascular growth resulted in improvements in myocardial perfusion after prolonged ischemia and protected from subsequent myocardial infarction. We further show that repetitive ischemia did not lead to increased expression of classic proangiogenic factors but instead resulted in activation of the innate immune system and recruitment of macrophages to growing blood vessels.
Conclusions: These studies describe a novel model of coronary angiogenesis and implicate the cardiac macrophage as a potential mediator of ischemia-driven coronary growth.
Keywords: collateral; coronary; coronary angiogenesis; macrophage; repetitive ischemia.
Figures







Similar articles
-
The essential role for endothelial cell sprouting in coronary collateral growth.J Mol Cell Cardiol. 2022 Apr;165:158-171. doi: 10.1016/j.yjmcc.2022.01.005. Epub 2022 Jan 22. J Mol Cell Cardiol. 2022. PMID: 35074317 Free PMC article.
-
Calpain inhibition improves collateral-dependent perfusion in a hypercholesterolemic swine model of chronic myocardial ischemia.J Thorac Cardiovasc Surg. 2016 Jan;151(1):245-52. doi: 10.1016/j.jtcvs.2015.08.101. Epub 2015 Sep 3. J Thorac Cardiovasc Surg. 2016. PMID: 26478238 Free PMC article.
-
Gene therapy for myocardial angiogenesis.Am Heart J. 1999 Aug;138(2 Pt 2):S132-41. doi: 10.1016/s0002-8703(99)70333-9. Am Heart J. 1999. PMID: 10426872 Review.
-
Cardioprotection during ischemia by coronary collateral growth.Am J Physiol Heart Circ Physiol. 2019 Jan 1;316(1):H1-H9. doi: 10.1152/ajpheart.00145.2018. Epub 2018 Oct 31. Am J Physiol Heart Circ Physiol. 2019. PMID: 30379567 Free PMC article. Review.
-
Reactive oxygen species drives myocardial angiogenesis?Antioxid Redox Signal. 2006 Nov-Dec;8(11-12):2161-8. doi: 10.1089/ars.2006.8.2161. Antioxid Redox Signal. 2006. PMID: 17034358 Review.
Cited by
-
A Unique Collateral Artery Development Program Promotes Neonatal Heart Regeneration.Cell. 2019 Feb 21;176(5):1128-1142.e18. doi: 10.1016/j.cell.2018.12.023. Epub 2019 Jan 24. Cell. 2019. PMID: 30686582 Free PMC article.
-
Myocardial B cells are a subset of circulating lymphocytes with delayed transit through the heart.JCI Insight. 2020 Feb 13;5(3):e134700. doi: 10.1172/jci.insight.134700. JCI Insight. 2020. PMID: 31945014 Free PMC article.
-
SerpinG1: A Novel Biomarker Associated With Poor Coronary Collateral in Patients With Stable Coronary Disease and Chronic Total Occlusion.J Am Heart Assoc. 2022 Dec 20;11(24):e027614. doi: 10.1161/JAHA.122.027614. Epub 2022 Dec 14. J Am Heart Assoc. 2022. PMID: 36515245 Free PMC article.
-
Resident cardiac macrophages mediate adaptive myocardial remodeling.Immunity. 2021 Sep 14;54(9):2072-2088.e7. doi: 10.1016/j.immuni.2021.07.003. Epub 2021 Jul 27. Immunity. 2021. PMID: 34320366 Free PMC article.
-
Long non‑coding RNA NORAD regulates angiogenesis of human umbilical vein endothelial cells via miR‑590‑3p under hypoxic conditions.Mol Med Rep. 2020 Jun;21(6):2560-2570. doi: 10.3892/mmr.2020.11064. Epub 2020 Apr 8. Mol Med Rep. 2020. PMID: 32323787 Free PMC article.
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013; 127:e6-e245 - PMC - PubMed
-
- Mukherjee D, Comella K, Bhatt DL, Roe MT, Patel V, Ellis SG. Clinical outcome of a cohort of patients eligible for therapeutic angiogenesis or transmyocardial revascularization. Am Heart J. 2001; 142:72-74 - PubMed
-
- Williams B, Menon M, Satran D, Hayward D, Hodges JS, Burke MN, Johnson RK, Poulose AK, Traverse JH, Henry TD. Patients with coronary artery disease not amenable to traditional revascularization: prevalence and 3‐year mortality. Catheter Cardiovasc Interv. 2010; 75:886-891 - PubMed
-
- Billinger M, Kloos P, Eberli FR, Windecker S, Meier B, Seiler C. Physiologically assessed coronary collateral flow and adverse cardiac ischemic events: a follow‐up study in 403 patients with coronary artery disease. J Am Coll Cardiol. 2002; 40:1545-1550 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
