

Outcomes among patients discharged from busy intensive care units
- PMID: 24081285
- PMCID: PMC4212937
- DOI: 10.7326/0003-4819-159-7-201310010-00004
Outcomes among patients discharged from busy intensive care units
Abstract
Background: Strains on the capacities of intensive care units (ICUs) may influence the quality of ICU-to-floor transitions.
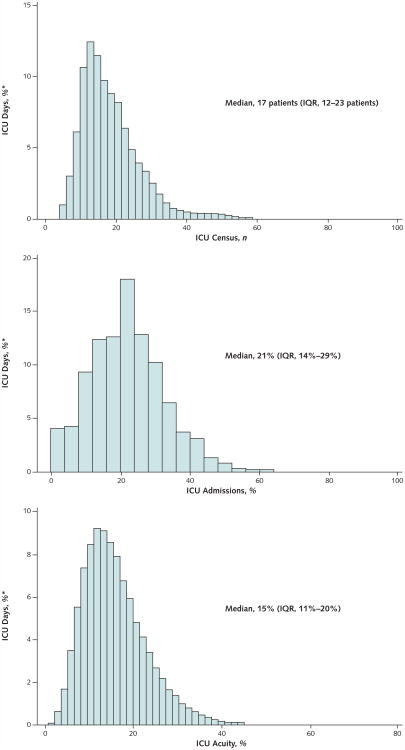
Objective: To determine how 3 metrics of ICU capacity strain (ICU census, new admissions, and average acuity) measured on days of patient discharges influence ICU length of stay (LOS) and post-ICU discharge outcomes.
Design: Retrospective cohort study from 2001 to 2008.
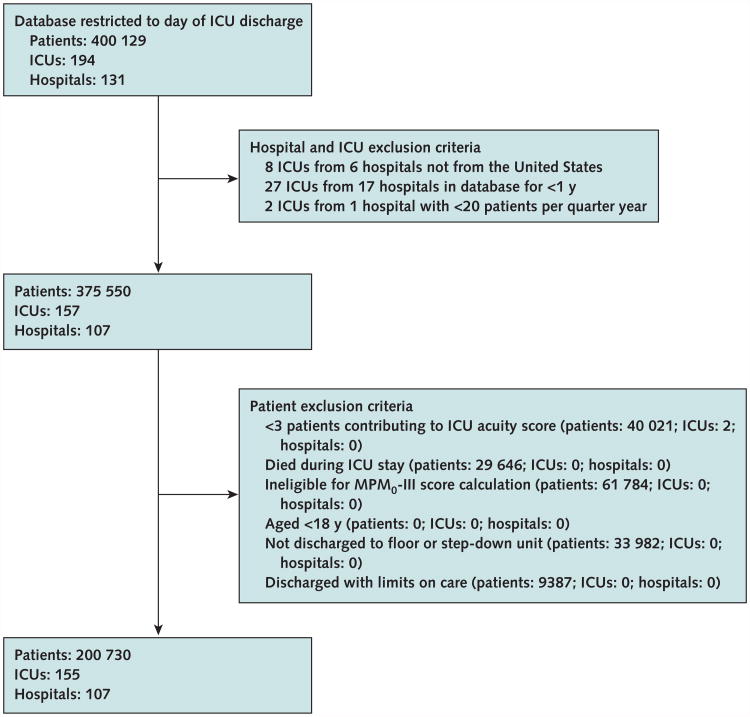
Setting: 155 ICUs in the United States.
Patients: 200 730 adults discharged from ICUs to hospital floors.
Measurements: Associations between ICU capacity strain metrics and discharged patient ICU LOS, 72-hour ICU readmissions, subsequent in-hospital death, post-ICU discharge LOS, and hospital discharge destination.
Results: Increases in the 3 strain variables on the days of ICU discharge were associated with shorter preceding ICU LOS (all P < 0.001) and increased odds of ICU readmissions (all P < 0.050). Going from the 5th to 95th percentiles of strain was associated with a 6.3-hour reduction in ICU LOS (95% CI, 5.3 to 7.3 hours) and a 1.0% increase in the odds of ICU readmission (CI, 0.6% to 1.5%). No strain variable was associated with increased odds of subsequent death, reduced odds of being discharged home from the hospital, or longer total hospital LOS.
Limitation: Long-term outcomes could not be measured.
Conclusion: When ICUs are strained, triage decisions seem to be affected such that patients are discharged from the ICU more quickly and, perhaps consequentially, have slightly greater odds of being readmitted to the ICU. However, short-term patient outcomes are unaffected. These results suggest that bed availability pressures may encourage physicians to discharge patients from the ICU more efficiently and that ICU readmissions are unlikely to be causally related to patient outcomes.
Primary funding source: Agency for Healthcare Research and Quality; National Heart, Lung, and Blood Institute; and Society of Critical Care Medicine.
Conflict of interest statement
Figures

References
-
- Kelley MA. Critical care workforce crisis: time to look in the mirror. Crit Care Med. 2008;36:1385–6. Editorial. - PubMed
-
- Halpern NA, Pastores SM, Greenstein RJ. Critical care medicine in the United States 1985-2000: an analysis of bed numbers, use, and costs. Crit Care Med. 2004;32:1254–9. - PubMed
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–62. - PubMed
-
- Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284:2762–70. - PubMed
-
- Kelley MA, Angus D, Chalfin DB, Crandall ED, Ingbar D, Johanson W, et al. The critical care crisis in the United States: a report from the profession. Chest. 2004;125:1514–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources