

Systemic sclerosis-associated pulmonary arterial hypertension
- PMID: 24081346
- PMCID: PMC3787920
- DOI: 10.1378/chest.12-2396
Systemic sclerosis-associated pulmonary arterial hypertension
Abstract
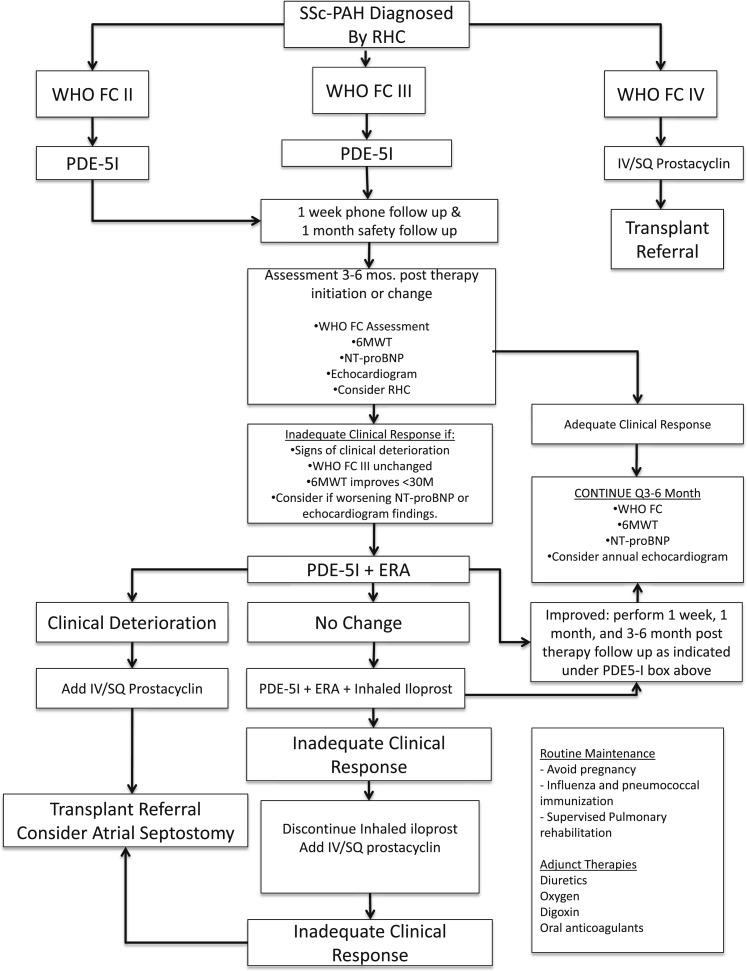
Pulmonary arterial hypertension (PAH) is the leading cause of death in systemic sclerosis (SSc) and affects up to 12% of all patients with SSc, with a 50% mortality rate within 3 years of PAH diagnosis. Compared with the idiopathic form of PAH (IPAH), patients with SSc-associated PAH (SSc-PAH) have a threefold increased risk of death and may receive a diagnosis late in the course of disease because of insidious onset and the high prevalence of cardiac, musculoskeletal, and pulmonary parenchymal comorbidities. Treatment with conventional forms of PAH therapy often yield poor results compared with IPAH cohorts; unfortunately, the exact reasons behind this remain poorly understood but likely include variations in the pathologic mechanisms, differences in cardiovascular response to increasing afterload, and inadequate strategies to detect and treat SSc-PAH early in its course. Current methods for screening and longitudinal evaluation of SSc-PAH, such as the 6-min walk test, transthoracic echocardiography, and MRI, each have notable advantages and disadvantages. We provide an up-to-date, focused review of SSc-PAH and how it differs from IPAH, including pathogenesis, appropriate screening for disease onset, and new approaches to treatment and longitudinal assessment of this disease.
Figures
References
-
- Jimenez SA, Derk CT. Following the molecular pathways toward an understanding of the pathogenesis of systemic sclerosis. Ann Intern Med. 2004;140(1):37-50 - PubMed
-
- Thenappan T, Shah SJ, Rich S, Gomberg-Maitland M. A USA-based registry for pulmonary arterial hypertension: 1982-2006. Eur Respir J. 2007;30(6):1103-1110 - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023-1030 - PubMed
-
- Fisher MR, Mathai SC, Champion HC, et al. Clinical differences between idiopathic and scleroderma-related pulmonary hypertension. Arthritis Rheum. 2006;54(9):3043-3050 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
