

The role of proinsulin and insulin in the diagnosis of insulinoma: a critical evaluation of the Endocrine Society clinical practice guideline
- PMID: 24081736
- PMCID: PMC3849676
- DOI: 10.1210/jc.2013-2182
The role of proinsulin and insulin in the diagnosis of insulinoma: a critical evaluation of the Endocrine Society clinical practice guideline
Abstract
Context: An end of fast insulin ≥ 3 μIU/mL and a proinsulin concentration ≥ 5 pmol/L have been suggested as useful cutoffs for the diagnosis of insulinoma.
Objective: The main objective was to evaluate the diagnostic performance of an end of fast insulin concentration ≥ 3 μIU/mL and an end of fast proinsulin concentration ≥ 5 pmol/L.
Design: The design was a case-control series.
Setting: The setting was a tertiary-care center.
Patients: Fifty-six subjects with a positive 48-hour supervised fast had an insulinoma between June 2000 and April 2011. During this same time period, a diagnosis of insulinoma was excluded in 29 subjects who underwent a supervised fast.
Intervention: 48-hour supervised fast.
Main outcome measure: The main outcome measures were serum insulin concentration and plasma proinsulin concentration.
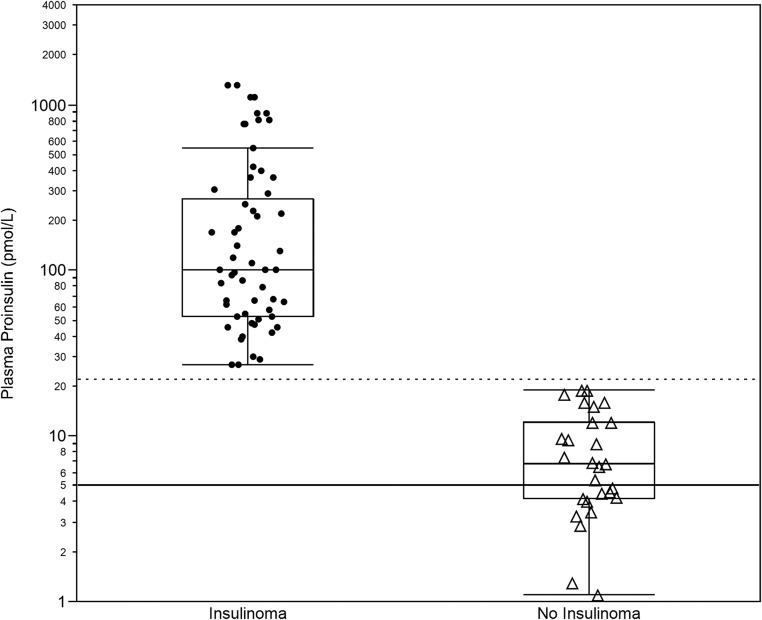
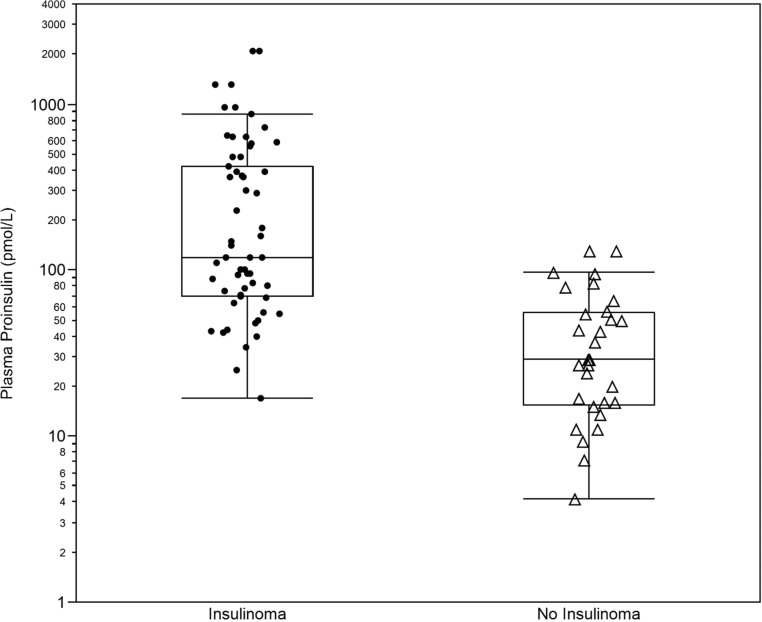
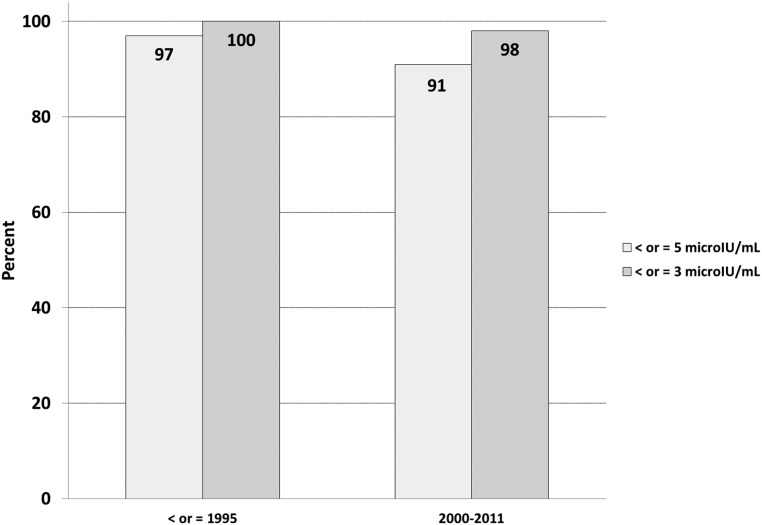
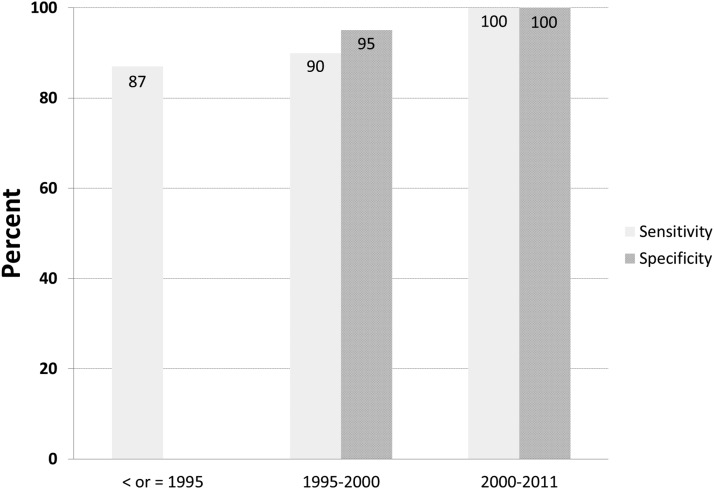
Results: Ninety-one percent of the patients with an insulinoma had a measured insulin concentration ≥5 μIU/mL at the end of fast. The sensitivity increased to 98% if the threshold to define inadequate insulin suppression was lowered to ≥3 μIU/mL. The median (interquartile range) end of fast proinsulin was 100 (53-270) pmol/L for cases and 6.8 (4.2-12.0) pmol/L for controls. An end of fast proinsulin value of ≥ 5 pmol/L could not distinguish cases from controls (59% false positive rate). All patients with an insulinoma (sensitivity 100%) and none of the control subject (specificity 100%) had end of fast proinsulin concentration ≥ 27 pmol/L.
Conclusions: Using a current insulin assay 9% of insulinoma cases end the supervised fast with an insulin concentration below 5 μIU/mL. Inadequate insulin suppression defined using a threshold of ≥ 3 μIU/mL increases the sensitivity of the test. The value of the proinsulin test lies in its unique ability to distinguish cases from controls. A proinsulin concentration of ≥22 pmol/L best discriminates cases from controls. Reliance on an end of fast proinsulin cutoff value of 5 pmol/L does not augment sensitivity but greatly reduces specificity of the test.
Figures
References
-
- Gorden P, Skarulis MC, Roach P, et al. Plasma proinsulin-like component in insulinoma: a 25-year experience. J Clin Endocrinol Metab. 1995;80(10):2884–2887 - PubMed
-
- Service FJ, McMahon MM, O'Brien PC, Ballard DJ. Functioning insulinoma—incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991;66(7):711–719 - PubMed
-
- Alsever RN, Roberts JP, Gerber JG, Mako ME, Rubenstein AH. Insulinoma with low circulating insulin levels: the diagnostic value of proinsulin measurements. Ann Intern Med. 1975;82(3):347–350 - PubMed
-
- Chia CW, Saudek CD. The diagnosis of fasting hypoglycemia due to an islet-cell tumor obscured by a highly specific insulin assay. J Clin Endocrinol Metab. 2003;88(4):1464–1467 - PubMed
-
- Gómez-Pérez FJ, Cuevas-Ramos D, Valdés PA, Aguilar-Salinas CA, Mehta R, Rull JA. Beta-cell adenomas without hyperinsulinemia with use of highly specific insulin radioimmunoassays: case report and review of literature. Endocr Pract. 2010;16(4):660–663 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
