

Impact of cardiovascular magnetic resonance on management and clinical decision-making in heart failure patients
- PMID: 24083836
- PMCID: PMC3851265
- DOI: 10.1186/1532-429X-15-89
Impact of cardiovascular magnetic resonance on management and clinical decision-making in heart failure patients
Erratum in
- J Cardiovasc Magn Reson. 2014;16:20
Abstract
Background: Cardiovascular magnetic resonance (CMR) can provide important diagnostic and prognostic information in patients with heart failure. However, in the current health care environment, use of a new imaging modality like CMR requires evidence for direct additive impact on clinical management. We sought to evaluate the impact of CMR on clinical management and diagnosis in patients with heart failure.
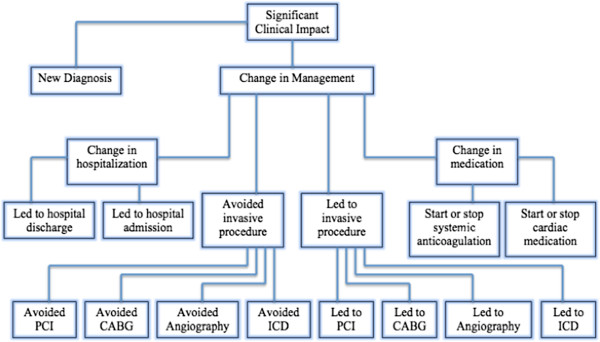
Methods: We prospectively studied 150 consecutive patients with heart failure and an ejection fraction ≤ 50% referred for CMR. Definitions for "significant clinical impact" of CMR were pre-defined and collected directly from medical records and/or from patients. Categories of significant clinical impact included: new diagnosis, medication change, hospital admission/discharge, as well as performance or avoidance of invasive procedures (angiography, revascularization, device therapy or biopsy).
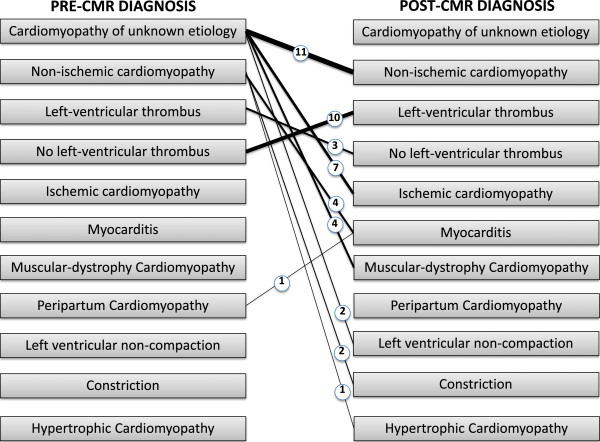
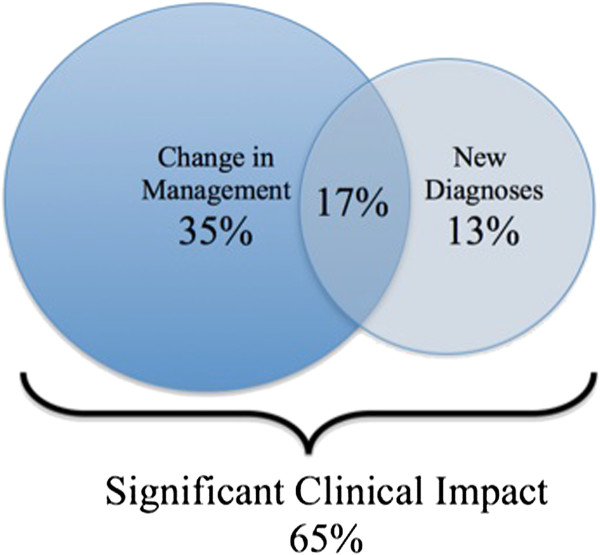
Results: Overall, CMR had a significant clinical impact in 65% of patients. This included an entirely new diagnosis in 30% of cases and a change in management in 52%. CMR results directly led to angiography in 9% and to the performance of percutaneous coronary intervention in 7%. In a multivariable model that included clinical and imaging parameters, presence of late gadolinium enhancement (LGE) was the only independent predictor of "significant clinical impact" (OR 6.72, 95% CI 2.56-17.60, p=0.0001).
Conclusions: CMR made a significant additive clinical impact on management, decision-making and diagnosis in 65% of heart failure patients. This additive impact was seen despite universal use of prior echocardiography in this patient group. The presence of LGE was the best independent predictor of significant clinical impact following CMR.
Figures
References
-
- Greenwood JP, Maredia N, Younger JF, Brown JM, Nixon J, Everett CC, Bijsterveld P, Ridgway JP, Radjenovic A, Dickinson CJ. et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial. Lancet. 2012;379(9814):453–60. doi: 10.1016/S0140-6736(11)61335-4. - DOI - PMC - PubMed
-
- Klem I, Heitner JF, Shah DJ, Sketch MH Jr, Behar V, Weinsaft J, Cawley P, Parker M, Elliott M, Judd RM. et al. Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhancement infarction imaging. J Am Coll Cardiol. 2006;47(8):1630–8. doi: 10.1016/j.jacc.2005.10.074. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
