

Predictors of response to tiotropium versus salmeterol in asthmatic adults
- PMID: 24084072
- PMCID: PMC3826080
- DOI: 10.1016/j.jaci.2013.08.003
Predictors of response to tiotropium versus salmeterol in asthmatic adults
Abstract
Background: Tiotropium has activity as an asthma controller. However, predictors of a positive response to tiotropium have not been described.
Objective: We sought to describe individual and differential responses of asthmatic patients to salmeterol and tiotropium when added to an inhaled corticosteroid, as well as predictors of a positive clinical response.
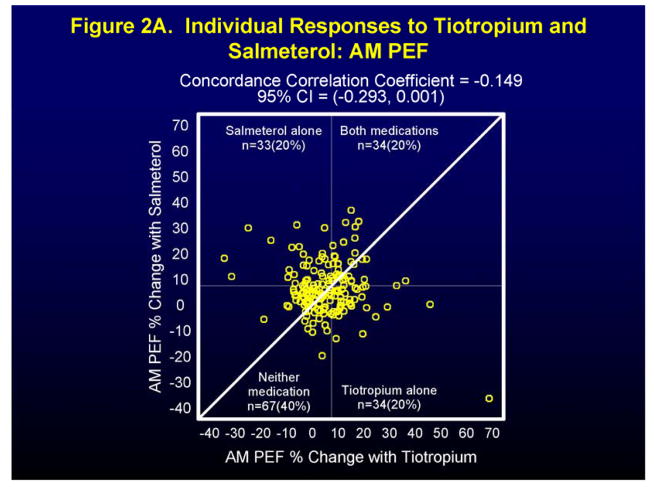
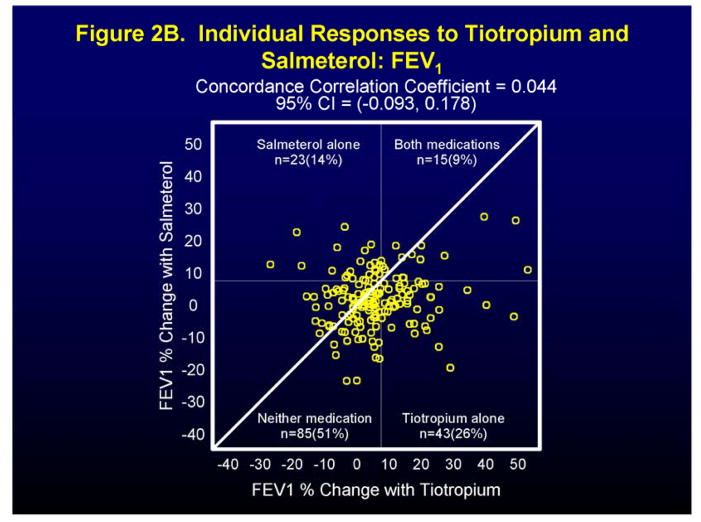
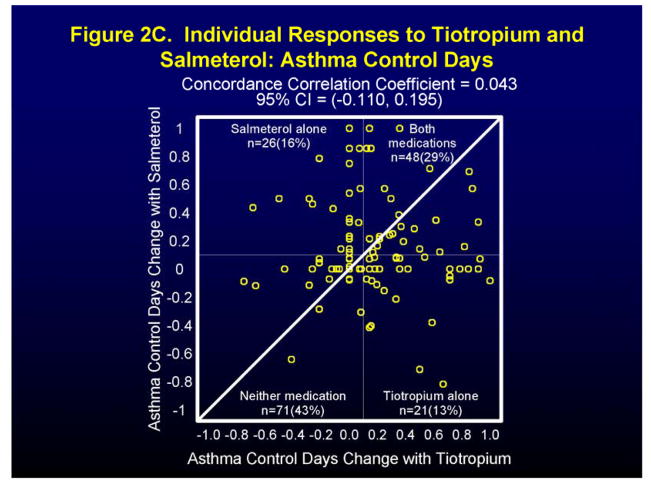
Methods: Data from the double-blind, 3-way, crossover National Heart, Lung, and Blood Institute's Asthma Clinical Research Network's Tiotropium Bromide as an Alternative to Increased Inhaled Glucocorticoid in Patients Inadequately Controlled on a Lower Dose of Inhaled Corticosteroid (ClinicalTrials.gov number, NCT00565266) trial were analyzed for individual and differential treatment responses to salmeterol and tiotropium and predictors of a positive response to the end points FEV1, morning peak expiratory flow (PEF), and asthma control days (ACDs).
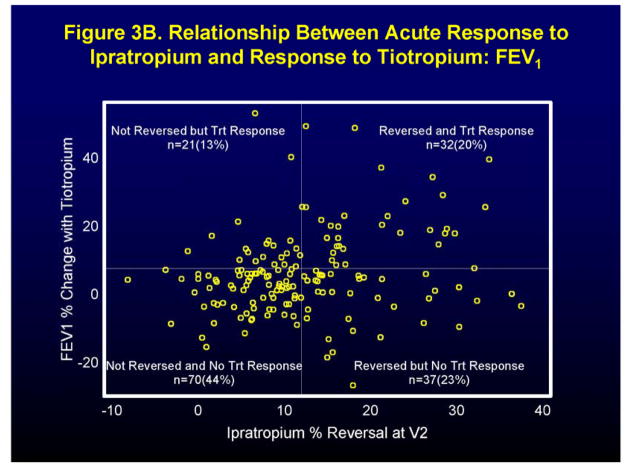
Results: Although approximately equal numbers of patients showed a differential response to salmeterol and tiotropium in terms of morning PEF (n = 90 and 78, respectively) and ACDs (n = 49 and 53, respectively), more showed a differential response to tiotropium for FEV1 (n = 104) than salmeterol (n = 62). An acute response to a short-acting bronchodilator, especially albuterol, predicted a positive clinical response to tiotropium for FEV1 (odds ratio, 4.08; 95% CI, 2.00-8.31; P < .001) and morning PEF (odds ratio, 2.12; 95% CI, 1.12-4.01; P = 0.021), as did a decreased FEV1/forced vital capacity ratio (FEV1 response increased 0.39% of baseline for every 1% decrease in FEV1/forced vital capacity ratio). Higher cholinergic tone was also a predictor, whereas ethnicity, sex, atopy, IgE level, sputum eosinophil count, fraction of exhaled nitric oxide, asthma duration, and body mass index were not.
Conclusion: Although these results require confirmation, predictors of a positive clinical response to tiotropium include a positive response to albuterol and airway obstruction, factors that could help identify appropriate patients for this therapy.
Keywords: ACD; ACRN; Asthma; Asthma Clinical Research Network; Asthma control day; FVC; Forced vital capacity; HFA; Hydrofluoroalkane; ICS; Inhaled corticosteroid; LABA; LAMA; Long-acting muscarinic antagonist; Long-acting β-agonist; NHLBI; National Heart, Lung, and Blood Institute; OR; Odds ratio; PEF; Peak expiratory flow; TALC; Tiotropium Bromide as an Alternative to Increased Inhaled Glucocorticoid in Patients Inadequately Controlled on a Lower Dose of Inhaled Corticosteroid (ClinicalTrials.gov number, NCT00565266) trial; predictor of response; responder analysis; salmeterol; tiotropium.
Copyright © 2013 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures


References
-
- National Asthma Education and Prevention Program. Expert Panel Report 3, Guidelines for the Diagnosis and Management of Asthma. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute; Bethesda, MD: 2007.
-
- Global Strategy for Asthma Management and Prevention. Global Initiative for Asthma (GINA); Available at: http://www.ginasthma.org.
-
- Weiss ST. New approaches to personalized medicine for asthma: where are we? J Allergy Clin Immunol. 2012;129:327–334. - PubMed
-
- Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, Wardlaw AJ, Pavord ID. Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet. 2002;360:1715–1721. - PubMed
-
- Greenberger PA. Personalized medicine for patients with asthma. J Allergy Clin Immunol. 2010;125:305–306. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
