

Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events--European Registry in Atrial Fibrillation (PREFER in AF)
- PMID: 24084680
- PMCID: PMC3864758
- DOI: 10.1093/europace/eut263
Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events--European Registry in Atrial Fibrillation (PREFER in AF)
Abstract
Aims: We sought to describe the management of patients with atrial fibrillation (AF) in Europe after the release of the 2010 AF Guidelines of the European Society of Cardiology.
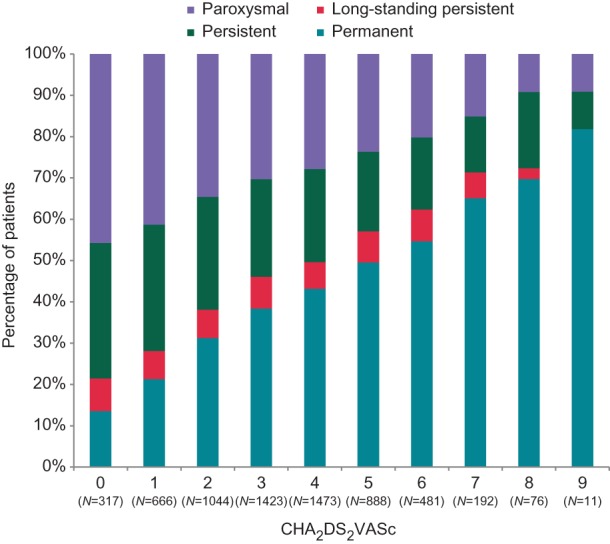
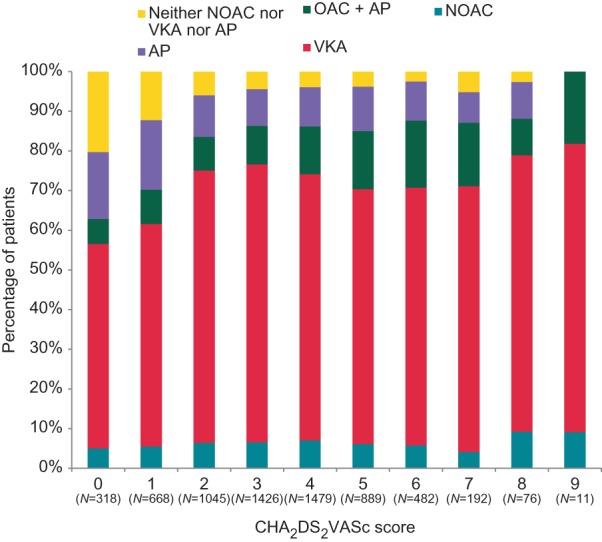
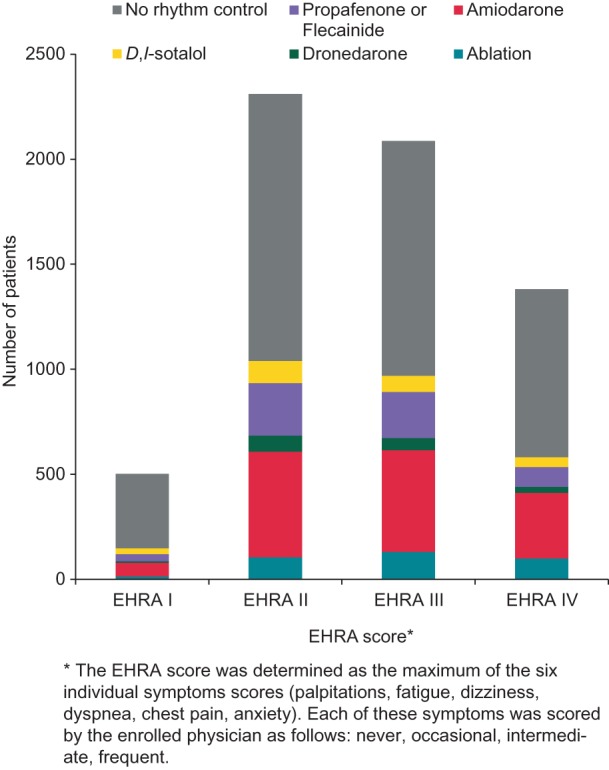
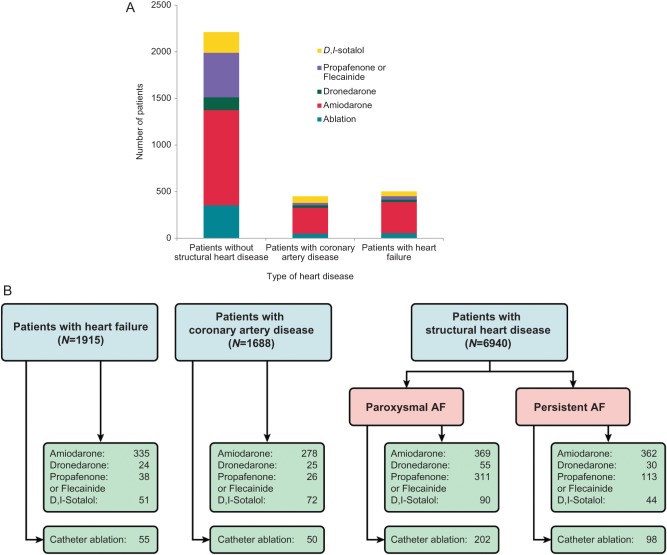
Methods and results: The PREFER in AF registry enrolled consecutive patients with AF from January 2012 to January 2013 in 461 centres in seven European countries. Seven thousand two hundred and forty-three evaluable patients were enrolled, aged 71.5 ± 11 years, 60.1% male, CHA2DS2VASc score 3.4 ± 1.8 (mean ± standard deviation). Thirty per cent patients had paroxysmal, 24.0% had persistent, 7.2% had long-standing persistent, and 38.8% had permanent AF. Oral anticoagulation was used in the majority of patients: 4799 patients (66.3%) received a vitamin K antagonist (VKA) as mono-therapy, 720 patients a combination of VKA and antiplatelet agents (9.9%), 442 patients (6.1%) a new oral anticoagulant drugs (NOAC). Antiplatelet agents alone were given to 808 patients (11.2%), no antithrombotic therapy to 474 patients (6.5%). Of 7034 evaluable patients, 5530 (78.6%) patients were adequately rate controlled (mean heart rate 60-100 bpm). Half of the patients (50.7%) received rhythm control therapy by electrical cardioversion (18.1%), pharmacological cardioversion (19.5%), antiarrhythmic drugs (amiodarone 24.1%, flecainide or propafenone 13.5%, sotalol 5.5%, dronedarone 4.0%), and catheter ablation (5.0%).
Conclusion: The management of AF patients in 2012 has adapted to recent evidence and guideline recommendations. Oral anticoagulant therapy with VKA (majority) or NOACs is given to over 80% of eligible patients, including those at risk for bleeding. Rate is often adequately controlled, and rhythm control therapy is widely used.
Keywords: Adherence to guidelines; Antiarrhythmic drugs; Anticoagulation; Atrial fibrillation; Catheter ablation; Guidelines; Management; Rate control; Registry; Rhythm control; Stroke.
Figures
Comment in
-
'Preferred' management of atrial fibrillation in Europe.Europace. 2014 Jan;16(1):1-3. doi: 10.1093/europace/eut270. Epub 2013 Sep 26. Europace. 2014. PMID: 24078343 No abstract available.
References
-
- Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27:949–53. - PubMed
-
- Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–6. - PubMed
-
- Kirchhof P, Lip GY, Van Gelder IC, Bax J, Hylek E, Kaab S, et al. Comprehensive risk reduction in patients with atrial fibrillation: emerging diagnostic and therapeutic options—a report from the 3rd Atrial Fibrillation Competence NETwork/European Heart Rhythm Association consensus conference. Europace. 2012;14:8–27. - PMC - PubMed
-
- Kirchhof P, Curtis AB, Skanes AC, Gillis AM, Samuel Wann L, John Camm A. Atrial fibrillation guidelines across the Atlantic: a comparison of the current recommendations of the European Society of Cardiology/European Heart Rhythm Association/European Association Of Cardiothoracic Surgeons, the American College of Cardiology Foundation/American Heart Association/Heart Rhythm Society, and the Canadian Cardiovascular Society. Eur Heart J. 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
