

Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women's Health Initiative randomized trials
- PMID: 24084921
- PMCID: PMC3963523
- DOI: 10.1001/jama.2013.278040
Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women's Health Initiative randomized trials
Abstract
Importance: Menopausal hormone therapy continues in clinical use but questions remain regarding its risks and benefits for chronic disease prevention.
Objective: To report a comprehensive, integrated overview of findings from the 2 Women's Health Initiative (WHI) hormone therapy trials with extended postintervention follow-up.
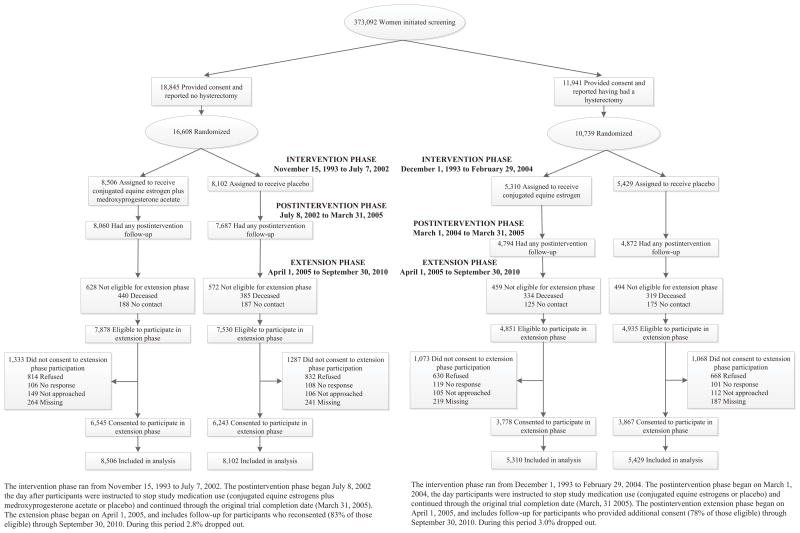
Design, setting, and participants: A total of 27,347 postmenopausal women aged 50 to 79 years were enrolled at 40 US centers.
Interventions: Women with an intact uterus received conjugated equine estrogens (CEE; 0.625 mg/d) plus medroxyprogesterone acetate (MPA; 2.5 mg/d) (n = 8506) or placebo (n = 8102). Women with prior hysterectomy received CEE alone (0.625 mg/d) (n = 5310) or placebo (n = 5429). The intervention lasted a median of 5.6 years in CEE plus MPA trial and 7.2 years in CEE alone trial with 13 years of cumulative follow-up until September 30, 2010.
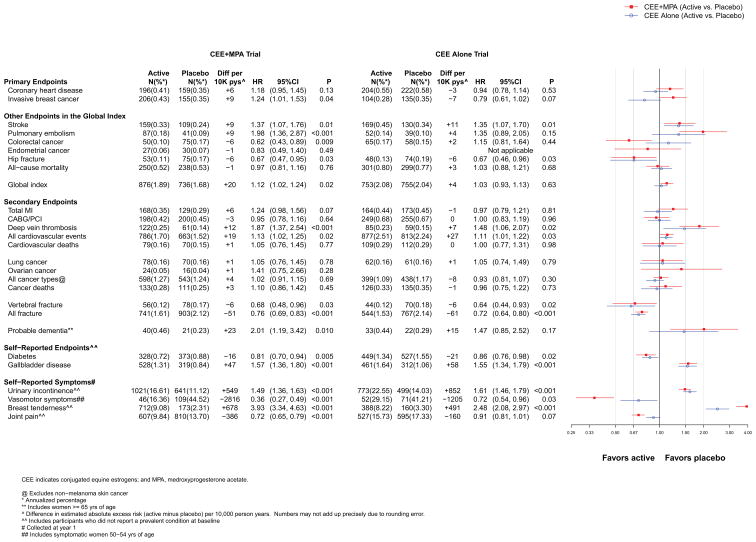
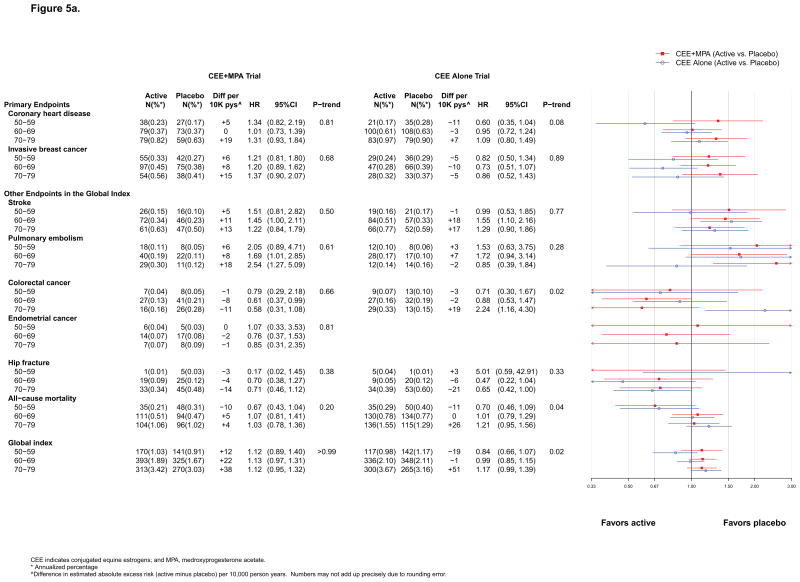
Main outcomes and measures: Primary efficacy and safety outcomes were coronary heart disease (CHD) and invasive breast cancer, respectively. A global index also included stroke, pulmonary embolism, colorectal cancer, endometrial cancer, hip fracture, and death.
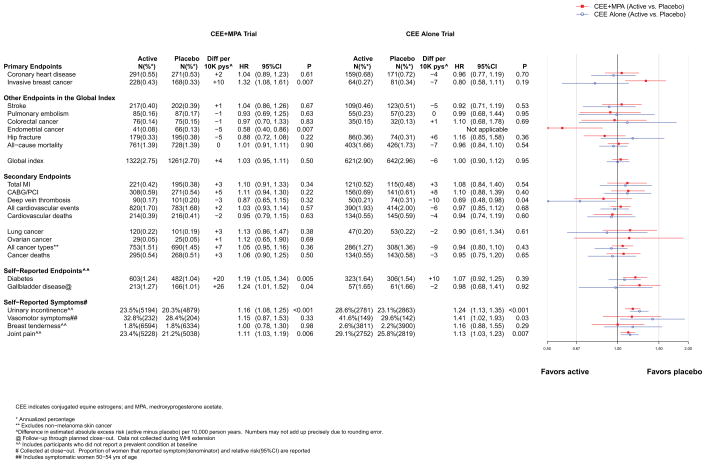
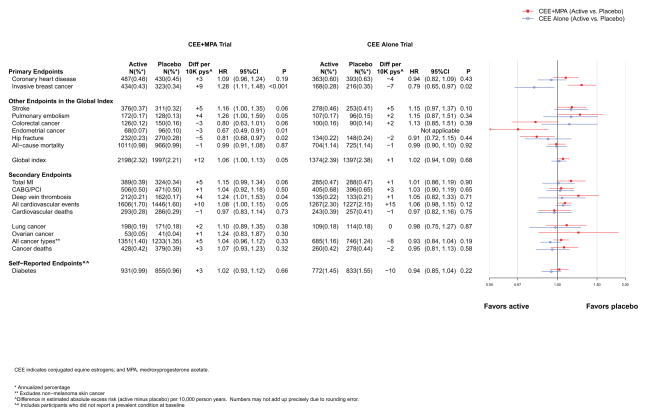
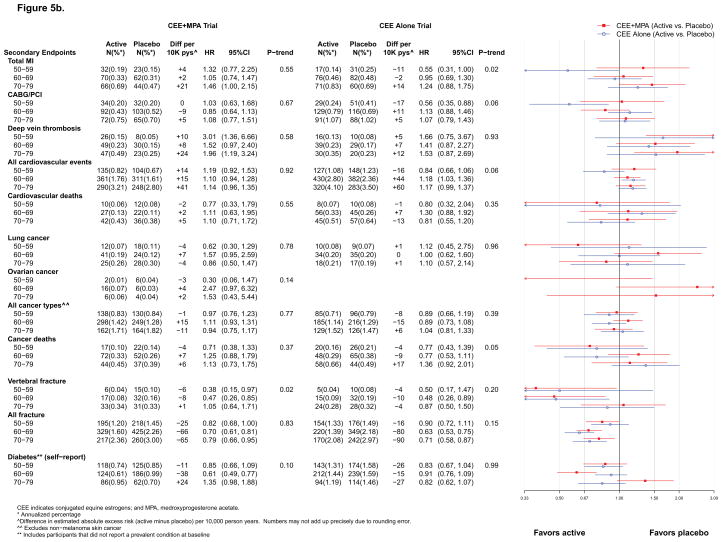
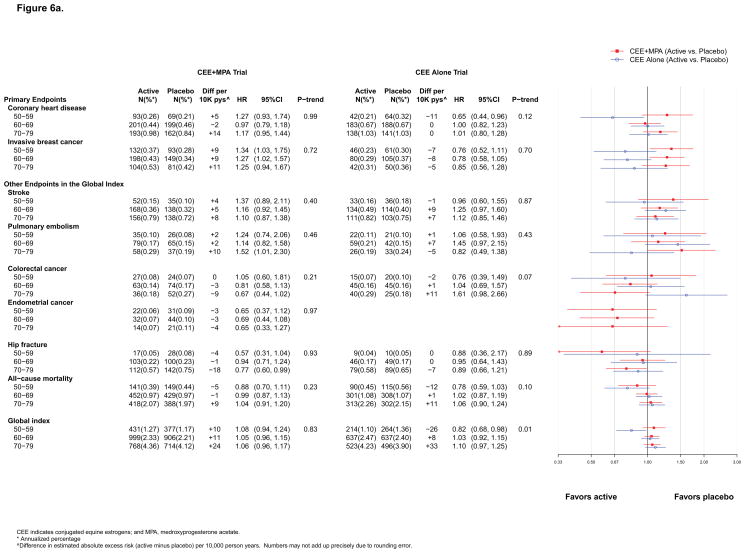
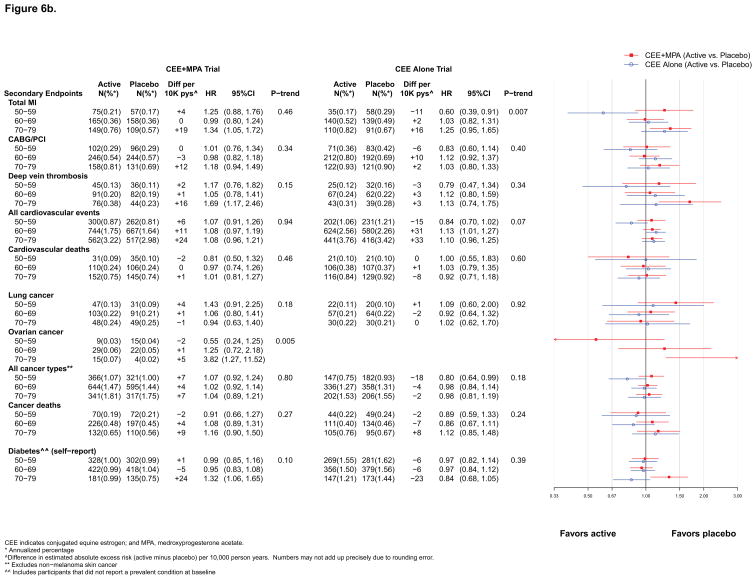
Results: During the CEE plus MPA intervention phase, the numbers of CHD cases were 196 for CEE plus MPA vs 159 for placebo (hazard ratio [HR], 1.18; 95% CI, 0.95-1.45) and 206 vs 155, respectively, for invasive breast cancer (HR, 1.24; 95% CI, 1.01-1.53). Other risks included increased stroke, pulmonary embolism, dementia (in women aged ≥65 years), gallbladder disease, and urinary incontinence; benefits included decreased hip fractures, diabetes, and vasomotor symptoms. Most risks and benefits dissipated postintervention, although some elevation in breast cancer risk persisted during cumulative follow-up (434 cases for CEE plus MPA vs 323 for placebo; HR, 1.28 [95% CI, 1.11-1.48]). The risks and benefits were more balanced during the CEE alone intervention with 204 CHD cases for CEE alone vs 222 cases for placebo (HR, 0.94; 95% CI, 0.78-1.14) and 104 vs 135, respectively, for invasive breast cancer (HR, 0.79; 95% CI, 0.61-1.02); cumulatively, there were 168 vs 216, respectively, cases of breast cancer diagnosed (HR, 0.79; 95% CI, 0.65-0.97). Results for other outcomes were similar to CEE plus MPA. Neither regimen affected all-cause mortality. For CEE alone, younger women (aged 50-59 years) had more favorable results for all-cause mortality, myocardial infarction, and the global index (nominal P < .05 for trend by age). Absolute risks of adverse events (measured by the global index) per 10,000 women annually taking CEE plus MPA ranged from 12 excess cases for ages of 50-59 years to 38 for ages of 70-79 years; for women taking CEE alone, from 19 fewer cases for ages of 50-59 years to 51 excess cases for ages of 70-79 years. Quality-of-life outcomes had mixed results in both trials.
Conclusions and relevance: Menopausal hormone therapy has a complex pattern of risks and benefits. Findings from the intervention and extended postintervention follow-up of the 2 WHI hormone therapy trials do not support use of this therapy for chronic disease prevention, although it is appropriate for symptom management in some women.
Trial registration: clinicaltrials.gov Identifier: NCT00000611.
Conflict of interest statement
Figures
Comment in
-
The Women's Health Initiative--a victory for women and their health.JAMA. 2013 Oct 2;310(13):1349-50. doi: 10.1001/jama.2013.278042. JAMA. 2013. PMID: 24084919 No abstract available.
-
Reproductive endocrinology: Hormone therapy to treat menopause--breaking a taboo.Nat Rev Endocrinol. 2014 Jan;10(1):6-8. doi: 10.1038/nrendo.2013.219. Epub 2013 Oct 29. Nat Rev Endocrinol. 2014. PMID: 24165999 No abstract available.
-
Hormone therapy use and outcomes in the Women's Health Initiative trials.JAMA. 2014 Jan 22-29;311(4):417. doi: 10.1001/jama.2013.285154. JAMA. 2014. PMID: 24449322 No abstract available.
-
Hormone therapy use and outcomes in the Women's Health Initiative trials--reply.JAMA. 2014 Jan 22-29;311(4):417-8. doi: 10.1001/jama.2013.285163. JAMA. 2014. PMID: 24449323 No abstract available.
-
Menopausal hormone therapy has risks and benefits during the intervention and poststopping phase.Evid Based Med. 2014 Jun;19(3):105. doi: 10.1136/eb-2013-101656. Epub 2014 Feb 3. Evid Based Med. 2014. PMID: 24492931 No abstract available.
-
Menopausal hormone therapy and prevention of chronic diseases: IMS members react to the recent JAMA paper.Climacteric. 2014 Feb;17(1):99-101. Climacteric. 2014. PMID: 24571029 No abstract available.
References
-
- Design of the Women’s Health Initiative clinical trial and observational study. The Women’s Health Initiative Study Group. Control Clin Trials. 1998;19(1):61–109. - PubMed
-
- Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–33. - PubMed
-
- Anderson GL, Limacher M, Assaf AR, Bassford T, Beresford SA, Black H, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701–12. - PubMed
-
- Guidelines for counseling postmenopausal women about preventive hormone therapy. American College of Physicians. Ann Intern Med. 1992;117(12):1038–41. - PubMed
-
- Grady D, Rubin SM, Petitti DB, Fox CS, Black D, Ettinger B, et al. Hormone therapy to prevent disease and prolong life in postmenopausal women. Ann Intern Med. 1992;117(12):1016–37. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01WH42112/WH/WHI NIH HHS/United States
- N01WH42119/WH/WHI NIH HHS/United States
- N01 WH022110/WH/WHI NIH HHS/United States
- N01WH42109/WH/WHI NIH HHS/United States
- N01WH42114/WH/WHI NIH HHS/United States
- N01WH32111/WH/WHI NIH HHS/United States
- N01WH42111/WH/WHI NIH HHS/United States
- N01WH42122/WH/WHI NIH HHS/United States
- N01WH44221/WH/WHI NIH HHS/United States
- N01WH42124/WH/WHI NIH HHS/United States
- N01WH32102/WH/WHI NIH HHS/United States
- N01WH32112/WH/WHI NIH HHS/United States
- N01WH32101/WH/WHI NIH HHS/United States
- N01WH32119/WH/WHI NIH HHS/United States
- N01WH32105/WH/WHI NIH HHS/United States
- N01WH42132/WH/WHI NIH HHS/United States
- N01WH42121/WH/WHI NIH HHS/United States
- N01 WH032109/WH/WHI NIH HHS/United States
- N01WH42113/WH/WHI NIH HHS/United States
- N01WH42125/WH/WHI NIH HHS/United States
- N01WH32106/WH/WHI NIH HHS/United States
- N01WH42129/WH/WHI NIH HHS/United States
- N01WH42108/WH/WHI NIH HHS/United States
- N01WH42118/WH/WHI NIH HHS/United States
- N01WH32113/WH/WHI NIH HHS/United States
- N01WH42120/WH/WHI NIH HHS/United States
- N01WH32118/WH/WHI NIH HHS/United States
- N01WH42131/WH/WHI NIH HHS/United States
- N01WH321115/WH/WHI NIH HHS/United States
- N01WH32122/WH/WHI NIH HHS/United States
- N01WH42107/WH/WHI NIH HHS/United States
- N01WH42130/WH/WHI NIH HHS/United States
- N01WH42117/WH/WHI NIH HHS/United States
- N01WH42115/WH/WHI NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- N01WH32109/WH/WHI NIH HHS/United States
- N01WH32108/WH/WHI NIH HHS/United States
- N01WH32100/WH/WHI NIH HHS/United States
- N01WH42123/WH/WHI NIH HHS/United States
- N01WH24152/WH/WHI NIH HHS/United States
- N01WH42110/WH/WHI NIH HHS/United States
- N01WH42126/WH/WHI NIH HHS/United States
- N01WH42116/WH/WHI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
