

Impact of ileostomy-related complications on the multidisciplinary treatment of rectal cancer
- PMID: 24085329
- PMCID: PMC4026258
- DOI: 10.1245/s10434-013-3287-9
Impact of ileostomy-related complications on the multidisciplinary treatment of rectal cancer
Abstract
Background: Radical resection is the primary treatment for rectal cancer. When anastomosis is possible, a temporary ileostomy is used to decrease morbidity from a poorly healed anastomosis. However, ileostomies are associated with complications, dehydration, and need for a second operation. We sought to evaluate the impact of ileostomy-related complications on the treatment of rectal cancer.
Methods: We conducted a retrospective study of patients who underwent sphincter-preserving surgery between January 2005 and December 2010 at a tertiary cancer center. The primary outcome was the overall rate of ileostomy-related complications. Secondary outcomes included complications related to ileostomy status, ileostomy closure, anastomotic complications at primary resection, rate of stoma closure, and completion of adjuvant chemotherapy assessed by multivariate logistic regression.
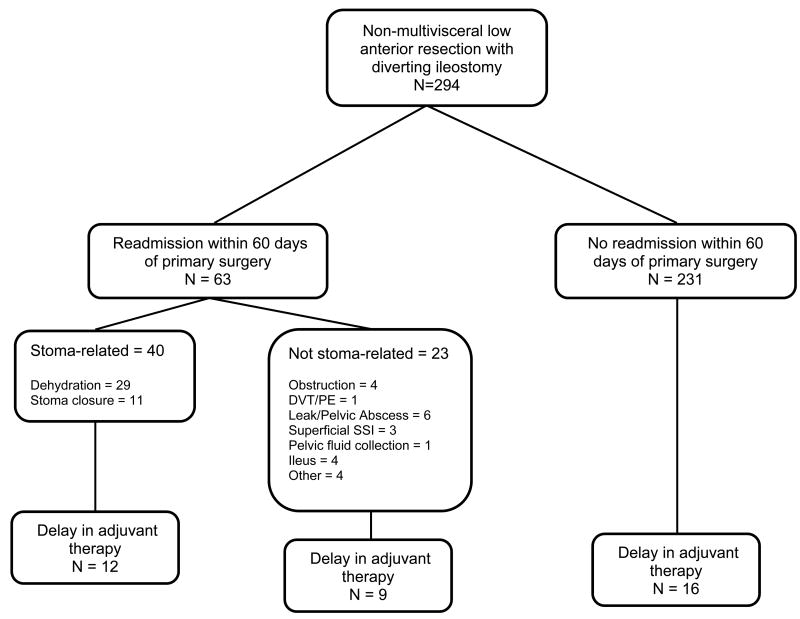
Results: Of 294 patients analyzed, 32% (n = 95) were women. Two hundred seventy-one (92%) received neoadjuvant chemoradiation. The median tumor distance from the anal verge was 7 cm (interquartile range 5-10 cm). Two hundred eighty-one (96%) underwent stoma closure at a median of 7 months (interquartile range 5.4-8.3 months). The most common complication related to readmission was dehydration (n = 32-11%). Readmission within 60 days of primary resection was associated with delay in initiating adjuvant chemotherapy (odds ratio 3.01, 95% confidence interval 1.42-6.38, p = 0.004).
Conclusions: Diverting ileostomies created during surgical treatment of rectal cancers are associated with morbidity; however, this is balanced against the risk of anastomosis-related morbidity at rectal resection. Given the potential benefit of fecal diversion, patient-oriented interventions to improve ostomy management, particularly during adjuvant chemotherapy, can be expected to yield marked benefits.
Figures
References
-
- Messaris E, Sehgal R, Deiling S, et al. Dehydration is the most common indication for readmission after diverting ileostomy creation. Diseases of the colon and rectum. 2012 Feb;55(2):175–180. - PubMed
-
- Beck-Kaltenbach N, Voigt K, Rumstadt B. Renal impairment caused by temporary loop ileostomy. International journal of colorectal disease. 2011 May;26(5):623–626. - PubMed
-
- Chow A, Tilney HS, Paraskeva P, Jeyarajah S, Zacharakis E, Purkayastha S. The morbidity surrounding reversal of defunctioning ileostomies: a systematic review of 48 studies including 6,107 cases. International journal of colorectal disease. 2009 Jun;24(6):711–723. - PubMed
-
- Bakx R, Busch OR, Bemelman WA, Veldink GJ, Slors JF, van Lanschot JJ. Morbidity of temporary loop ileostomies. Digestive surgery. 2004;21(4):277–281. - PubMed
-
- Carlsen E, Bergan AB. Loop ileostomy: technical aspects and complications. The European journal of surgery = Acta chirurgica. 1999 Feb;165(2):140–143. discussion 144. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
