

Opportunistic infections--coming to the limits of immunosuppression?
- PMID: 24086067
- PMCID: PMC3784816
- DOI: 10.1101/cshperspect.a015669
Opportunistic infections--coming to the limits of immunosuppression?
Abstract
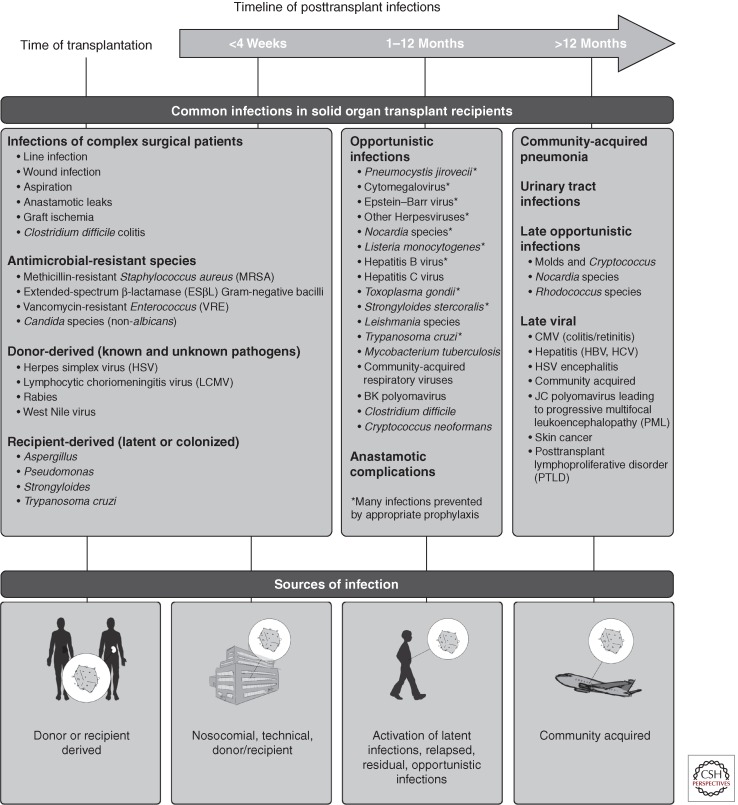
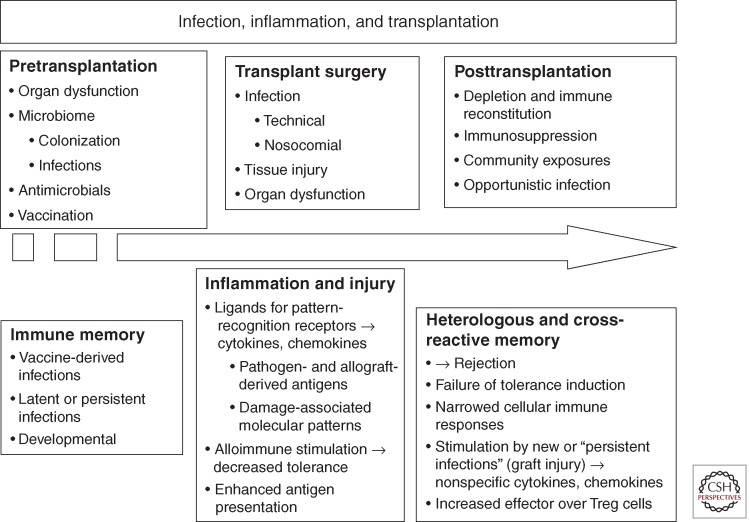
Possible etiologies of infection in the solid organ recipient are diverse, ranging from common bacterial and viral pathogens to opportunistic pathogens that cause invasive disease only in immunocompromised hosts. The recognition of infectious syndromes in this population is limited by alterations in the clinical manifestations by immunosuppression. The risk of serious infections in the organ transplant patient is determined by the interaction between the patients' recent and distant epidemiological exposures and all factors that contribute to the patient's net state of immune suppression. This risk is altered by antimicrobial prophylaxis and changes in immunosuppressive therapies. In addition to the direct effects of infection, opportunistic infections, and the microbiome may adversely shape the host immune responses with diminished graft and patient survivals. Antimicrobial therapies are more complex than in the normal host with a significant incidence of drug toxicity and a propensity for drug interactions with the immunosuppressive agents used to maintain graft function. Rapid and specific microbiologic diagnosis is essential. Newer microbiologic assays have improved the diagnosis and management of opportunistic infections. These tools coupled with assays that assess immune responses to infection and to graft antigens may allow optimization of management for graft recipients in the future.
Figures
References
-
- Adams AB, Pearson TC, Larsen CP 2003a. Heterologous immunity: An overlooked barrier to tolerance. Immunol Rev 196: 147–160 - PubMed
-
- Avery RK 2006. Infections after lung transplantation. Semin Respir Crit Care Med 27: 544–551 - PubMed
-
- Bando K, Paradis IL, Komatsu K, Konishi H, Matsushima M, Keena RJ, Hardesty RL, Armitage JM, Griffith BP 1995. Analysis of time-dependent risks for infection, rejection, and death after pulmonary transplantation. J Thorac Cardiovasc Surg 109: 49–57; discussion 57-49 - PubMed
-
- Biswas R, Tabor E, Hsia CC, Wright DJ, Laycock ME, Fiebig EW, Peddada L, Smith R, Schreiber GB, Epstein JS, et al. 2003. Comparative sensitivity of HBV NATs and HBsAg assays for detection of acute HBV infection. Transfusion 43: 788–798 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical