

Adrenocortical carcinoma: clinical outcomes and prognosis of 330 patients at a tertiary care center
- PMID: 24086089
- PMCID: PMC4441210
- DOI: 10.1530/EJE-13-0519
Adrenocortical carcinoma: clinical outcomes and prognosis of 330 patients at a tertiary care center
Abstract
Objective: Adrenocortical carcinoma (ACC) is a rare malignancy with a poor prognosis. Herein, we describe the clinical features and outcomes for a large series of ACC patients.
Design and methods: Retrospective review of ACC patients seen at The University of Texas MD Anderson Cancer Center from 1998 through 2011.
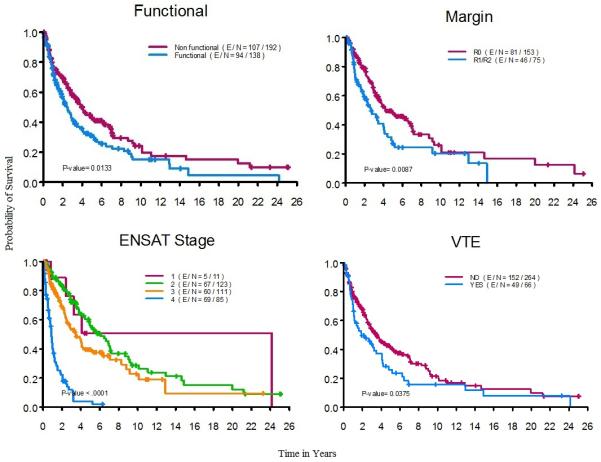
Results: A total of 330 patients with median age at diagnosis of 48.5 years; 12 (3.6%) patients were under 18 years. Hormonally functioning tumors represented 41.8% (n=138) of all cases. Surgical resection for the primary tumor was done in 275 (83.3%) patients (45 at MD Anderson (16.4%)). For those who had surgical resection, the median local-recurrence-free time was 1.04 years. Factors associated with local recurrence included positive surgical margins (P=0.007) and advanced disease stage (P=0.026). Median overall survival time for all patients was 3.21 years. Median survival times were 24.1, 6.08, 3.47, and 0.89 years for stages I, II, III, and IV respectively. In multivariable analysis, older age, functioning tumors, and higher disease stage remained significant prognostic factors associated with poor survival.
Conclusion: ACC prognosis remains poor with the use of currently available treatments. Older age, functioning tumors, and incomplete resections are clinical factors associated with poor survival. Surgical expertise is important to achieve complete resections and to improve outcome.
Figures

References
-
- Gerhardt PR, Handy VH, Ferber B. Trends in cancer incidence, mortality, and probability in the state of New York. N Y State J Med. 1957;57:1387–1390. - PubMed
-
- Griswold MH, Cutler SJ. The Connecticut cancer register. Seventeen years of experience. 1956. Conn Med. 2006;70:323–328. - PubMed
-
- Soreide JA, Brabrand K, Thoresen SO. Adrenal cortical carcinoma in Norway, 1970-1984. World J Surg. 1992;16:663–667. discussion 668. - PubMed
-
- Nader S, Hickey RC, Sellin RV, Samaan NA. Adrenal cortical carcinoma. A study of 77 cases. Cancer. 1983;52:707–711. - PubMed
-
- Vassilopoulou-Sellin R, Schultz PN. Adrenocortical carcinoma. Clinical outcome at the end of the 20th century. Cancer. 2001;92:1113–1121. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
