

"Best practice" skills lab training vs. a "see one, do one" approach in undergraduate medical education: an RCT on students' long-term ability to perform procedural clinical skills
- PMID: 24086732
- PMCID: PMC3783438
- DOI: 10.1371/journal.pone.0076354
"Best practice" skills lab training vs. a "see one, do one" approach in undergraduate medical education: an RCT on students' long-term ability to perform procedural clinical skills
Abstract
Background: Benefits of skills lab training are widely accepted, but there is sparse research on its long-term effectiveness. We therefore conducted a prospective, randomised controlled-trial to investigate whether in a simulated setting students trained according to a "best practice" model (BPSL) perform two skills of different complexity (nasogastral tube insertion, NGT; intravenous cannulation, IVC) better than students trained with a traditional "see one, do one" teaching approach (TRAD), at follow-up of 3 or 6 months.
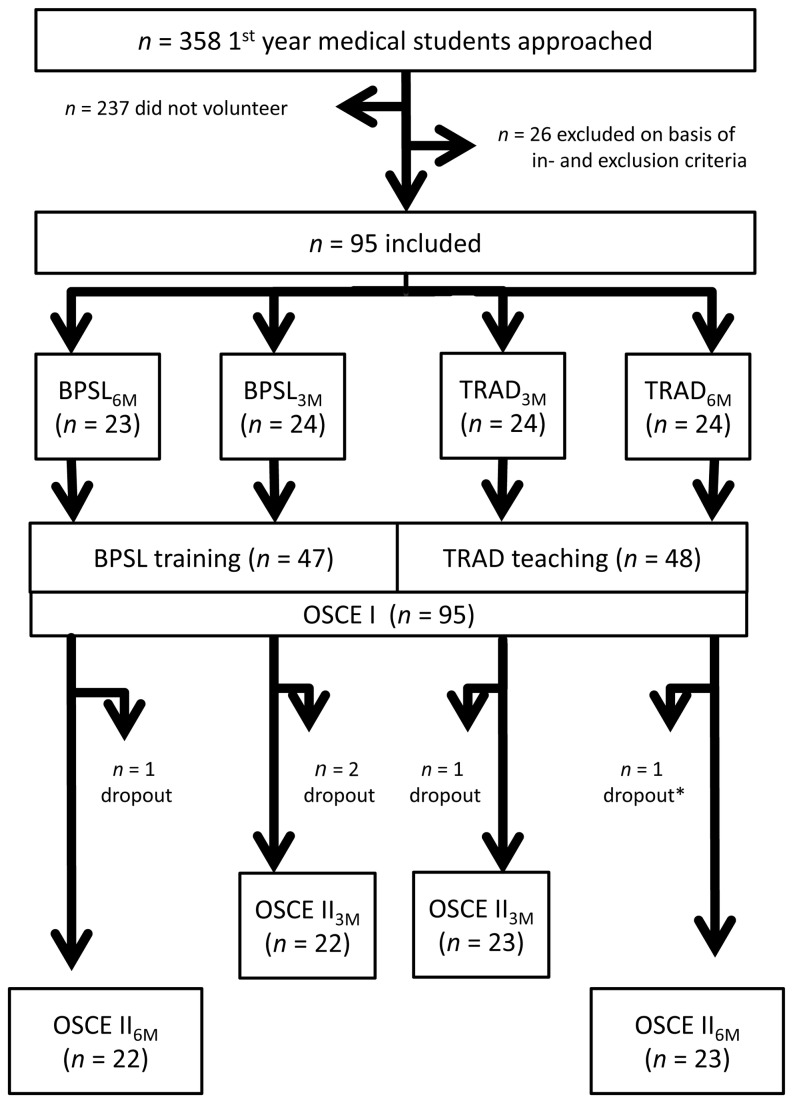
Methodology and principal findings: 94 first-year medical students were randomly assigned to one of four groups: BPSL training or TRAD teaching with follow-up at 3 (3M) or 6 (6M) months. BPSL included structured feedback, practice on manikins, and Peyton's "Four-Step-Approach", while TRAD was only based on the "see one - do one" principle. At follow-up, manikins were used to assess students' performance by two independent blinded video-assessors using binary checklists and a single-item global assessment scale. BPSL students scored significantly higher immediately after training (NGT: BPSL3M 94.8%±0.2 and BPSL6M 95.4%±0.3 percentage of maximal score ± SEM; TRAD3M 86.1%±0.5 and TRAD6M 84.7%±0.4. IVC: BPSL3M 86.4%±0.5 and BPSL6M 88.0%±0.5; TRAD3M 73.2%±0.7 and TRAD6M 72.5%±0.7) and lost significantly less of their performance ability at each follow-up (NGT: BPSL3M 86.3%±0.3 and TRAD3M 70.3%±0.6; BPSL6M 89.0%±0.3 and TRAD6M 65.4%±0.6; IVC: BPSL3M 79.5%±0.5 and TRAD3M 56.5%±0.5; BPSL6M 73.2%±0.4 and TRAD6M 51.5%±0.8). In addition, BPSL students were more often rated clinically competent at all assessment times. The superiority at assessment after training was higher for the more complex skill (IVC), whereas NGT with its lower complexity profited more with regard to long-term retention.
Conclusions: This study shows that within a simulated setting BPSL is significantly more effective than TRAD for skills of different complexity assessed immediately after training and at follow-up. The advantages of BPSL training are seen especially in long-term retention.
Conflict of interest statement
Figures


References
-
- Ziv A, Ben-David S, Ziv M (2005) Simulation based medical education: an opportunity to learn from errors. Med Teach 27: 193-199. doi:10.1080/01421590500126718. PubMed: 16011941. - DOI - PubMed
-
- Barrows HS (1993) An overview of the uses of standardized patients for teaching and evaluating clinical skills. AAMC. Acad Med J Assoc Am Med Colleges 68: 443-451; discussion 451-443 doi:10.1097/00001888-199306000-00002. - DOI - PubMed
-
- Bradley P, Postlethwaite K (2003) Setting up a clinical skills learning facility. Med Educ 37 Suppl 1: 6-13. doi:10.1046/j.1365-2923.37.s1.11.x. - DOI - PubMed
-
- Nikendei C, Zeuch A, Dieckmann P, Roth C, Schäfer S et al. (2005) Role-playing for more realistic technical skills training. Med Teach 27: 122-126. doi:10.1080/01421590400019484. PubMed: 16019330. - DOI - PubMed
-
- Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ (2005) Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach 27: 10-28. doi:10.1080/01421590500046924. PubMed: 16147767. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
