

Early treatment with IgM-enriched intravenous immunoglobulin does not mitigate critical illness polyneuropathy and/or myopathy in patients with multiple organ failure and SIRS/sepsis: a prospective, randomized, placebo-controlled, double-blinded trial
- PMID: 24088271
- PMCID: PMC4056097
- DOI: 10.1186/cc13028
Early treatment with IgM-enriched intravenous immunoglobulin does not mitigate critical illness polyneuropathy and/or myopathy in patients with multiple organ failure and SIRS/sepsis: a prospective, randomized, placebo-controlled, double-blinded trial
Abstract
Introduction: Critical illness polyneuropathy and/or myopathy (CIPNM) is a severe complication of critical illness. Retrospective data suggest that early application of IgM-enriched intravenous immunoglobulin (IVIG) may prevent or mitigate CIPNM. Therefore, the primary objective was to assess the effect of early IgM-enriched IVIG versus placebo to mitigate CIPNM in a prospective setting.
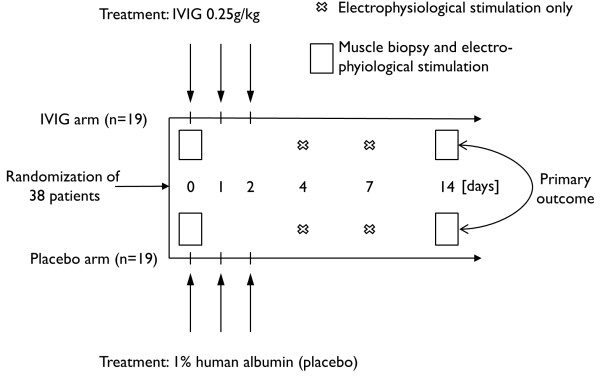
Methods: In this prospective, randomized, double-blinded and placebo-controlled trial, 38 critically ill patients with multiple organ failure (MOF), systemic inflammatory response syndrome (SIRS)/sepsis, and early clinical signs of CIPNM were included. Patients were randomly assigned to be treated either with IgM-enriched IVIG or placebo over a period of three days. CIPNM was measured by the CIPNM severity sum score based on electrophysiological stimulation of the median, ulnar, and tibial nerves on days 0, 4, 7, 14 and on the histological evaluation of muscle biopsies on days 0 and 14 and ranged from 0 (no CIPNM) to 8 (very severe CIPNM).
Results: A total of 38 critically ill patients were included and randomized to receive either IgM-enriched IVIG (n = 19) or placebo (n = 19). Baseline characteristics were similar between the two groups. CIPNM could not be improved by IVIG treatment, represented by similar CIPNM severity sum scores on day 14 (IVIG vs. placebo: 4.8 ± 2.0 vs. 4.5 ± 1.8; P = 0.70). CIPNM severity sum score significantly increased from baseline to day 14 (3.5 ± 1.6 vs. 4.6 ± 1.9; P = 0.002). After an interim analysis the study was terminated early due to futility in reaching the primary endpoint.
Conclusions: Early treatment with IVIG did not mitigate CIPNM in critically ill patients with MOF and SIRS/sepsis.
Trial registration: Clinicaltrials.gov: NCT01867645.
Figures


References
-
- De Letter MA, van Doorn PA, Savelkoul HF, Laman JD, Schmitz PI, Op de Coul AA, Visser LH, Kros JM, Teepen JL, van der Meché FG. Critical illness polyneuropathy and myopathy (CIPNM): evidence for local immune activation by cytokine-expression in the muscle tissue. J Neuroimmunol. 2000;17:206–213. doi: 10.1016/S0165-5728(99)00252-0. - DOI - PubMed
-
- Garnacho-Montero J, Madrazo-Osuna J, Garcia-Garmendia JL, Ortiz-Leyba C, Jimenez-Jimenez FJ, Barrero-Almodovar A, Garnacho-Montero MC, Moyano-Del-Estad MR. Critical illness polyneuropathy: risk factors and clinical consequences. A cohort study in septic patients. Intensive Care Med. 2001;17:1288–1296. doi: 10.1007/s001340101009. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
