

Prehospital hypertonic saline resuscitation attenuates the activation and promotes apoptosis of neutrophils in patients with severe traumatic brain injury
- PMID: 24088993
- PMCID: PMC3913169
- DOI: 10.1097/SHK.0000000000000038
Prehospital hypertonic saline resuscitation attenuates the activation and promotes apoptosis of neutrophils in patients with severe traumatic brain injury
Abstract
Background: Activation of polymorphonuclear neutrophils (PMNs) is thought to contribute to traumatic brain injury (TBI). Since hypertonic fluids can inhibit PMN activation, we studied whether hypertonic fluid resuscitation can reduce excessive PMN activation in TBI patients.
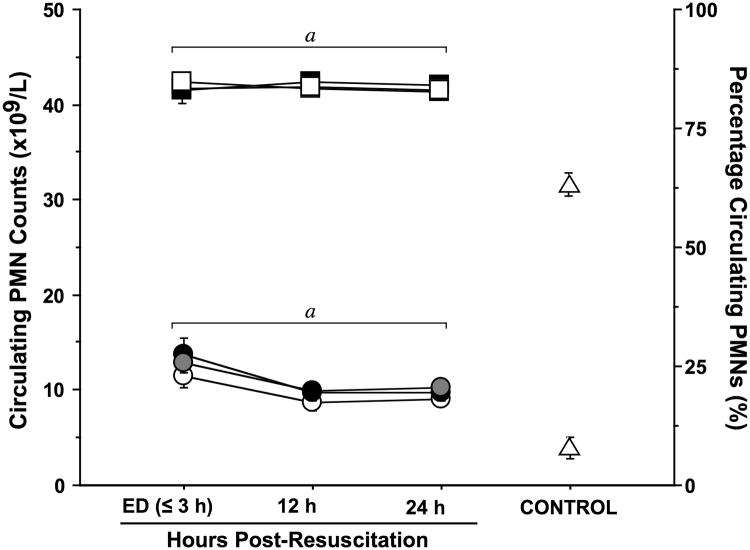
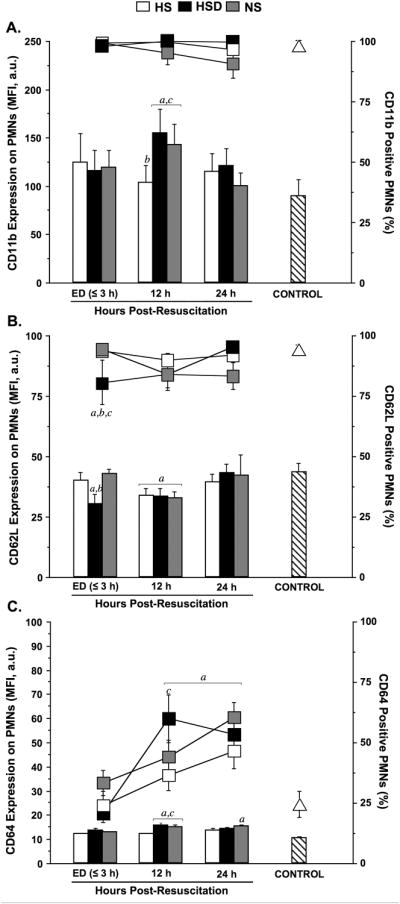
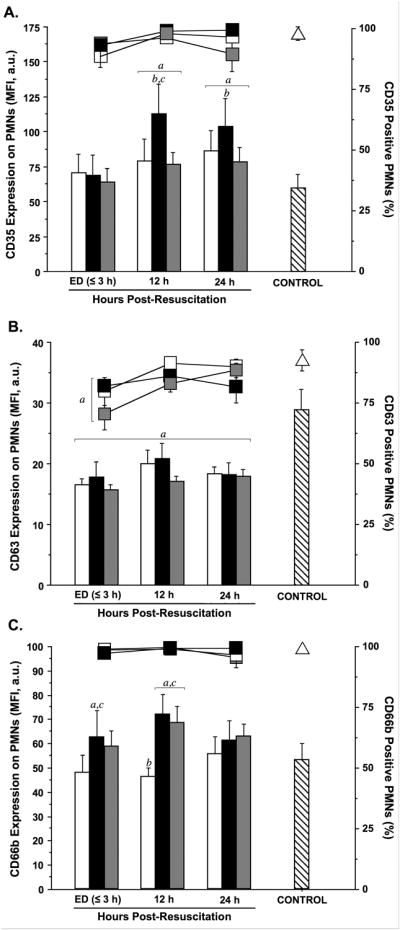
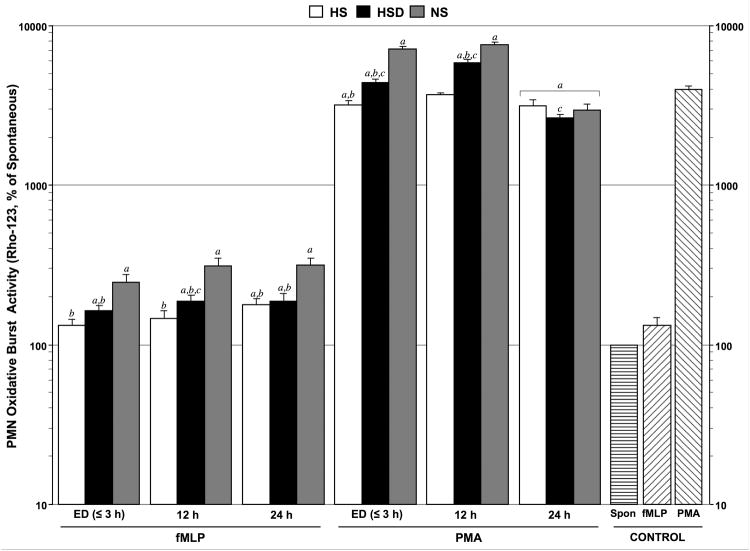
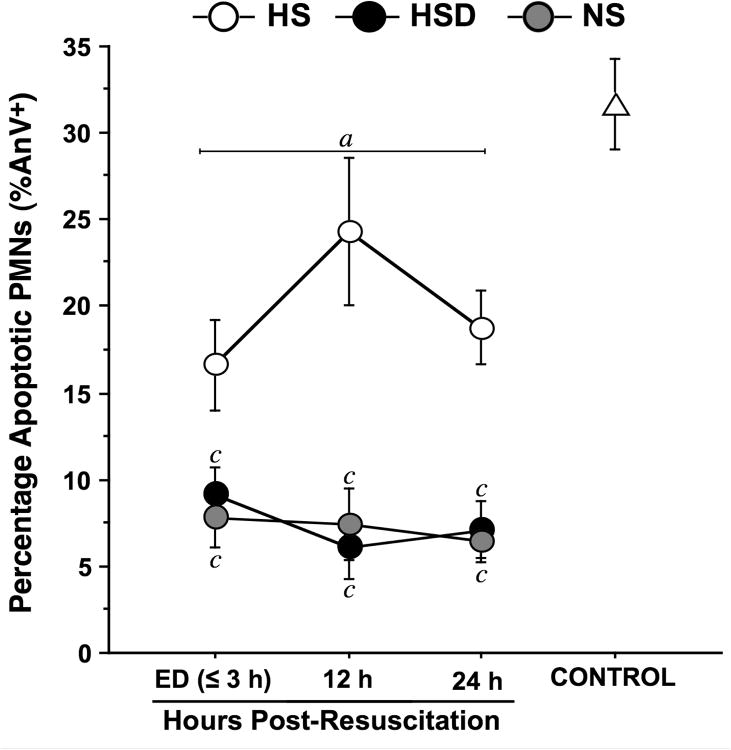
Methods: Trauma patients with severe TBI were resuscitated with 250 mL of either 7.5% hypertonic saline (HS; n = 22), HS + 6% dextran-70 (HSD; n = 22), or 0.9% normal saline (NS; n = 39), and blood samples were collected on hospital admission and 12 and 24 h after resuscitation. Polymorphonuclear neutrophil activation (CD11b, CD62L, CD64) and degranulation (CD63, CD66b, CD35) markers and oxidative-burst activity, as well as spontaneous PMN apoptosis were measured by flow cytometry.
Results: Relative to healthy controls, TBI patients showed increased PMN activation and decreased apoptosis of PMNs. In the HS group, but not in the HSD group, markers of PMN adhesion (CD11b, CD64) and degranulation (CD35, CD66b) were significantly lower than those in the NS group. These effects were particularly pronounced 12 h after resuscitation. Treatment with HS and HSD inhibited PMN oxidative burst responses compared with NS-treated patients. Hypertonic saline alone partially restored delayed PMN apoptosis. Despite these differences, the groups did not differ in clinical outcome parameters such as mortality and Extended Glasgow Outcome Scale.
Conclusions: This study demonstrates that prehospital resuscitation with HS can partially restore normal PMN activity and the apoptotic behavior of PMNs, whereas resuscitation with HSD was largely ineffective. Although the results are intriguing, additional research will be required to translate these effects of HS into treatment strategies that improve clinical outcome in TBI patients.
Figures
References
-
- Maas AI, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults. Lancet Neurol. 2008;7:728–41. - PubMed
-
- Stein SC, Georgoff P, Meghan S, Mizra K, Sonnad SS. 150 years of treating severe traumatic brain injury: a systematic review of progress in mortality. J Neurotrauma. 2010;27:1343–53. - PubMed
-
- Smania N, Avesani R, Roncari L, Ianes P, Girardi P, Varalta V, Gambini MG, Fiaschi A, Gandolfi M. Factors predicting functional and cognitive recovery following severe traumatic, anoxic, and cerebrovascular brain damage. J Head Trauma Rehabil. 2013;28:131–40. - PubMed
-
- Werner C, Engelhard K. Pathophysiology of traumatic brain injury. Br J Anaesth. 2007;99:4–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- R01 GM060475/GM/NIGMS NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- R01 GM051477/GM/NIGMS NIH HHS/United States
- R29 GM051477/GM/NIGMS NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- AI-080582/AI/NIAID NIH HHS/United States
- R01 AI072287/AI/NIAID NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- GM-51477/GM/NIGMS NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- GM-60475/GM/NIGMS NIH HHS/United States
- AI-072287/AI/NIAID NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- R01 AI080582/AI/NIAID NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
