

Quantified pathologic response assessed as residual tumor burden is a predictor of recurrence-free survival in patients with rectal cancer who undergo resection after neoadjuvant chemoradiotherapy
- PMID: 24089344
- PMCID: PMC5897128
- DOI: 10.1002/cncr.28331
Quantified pathologic response assessed as residual tumor burden is a predictor of recurrence-free survival in patients with rectal cancer who undergo resection after neoadjuvant chemoradiotherapy
Abstract
Background: The current study was conducted to determine whether quantified pathologic response assessed as a percentage of residual tumor cells is predictive of recurrence-free survival (RFS) in patients with rectal cancer.
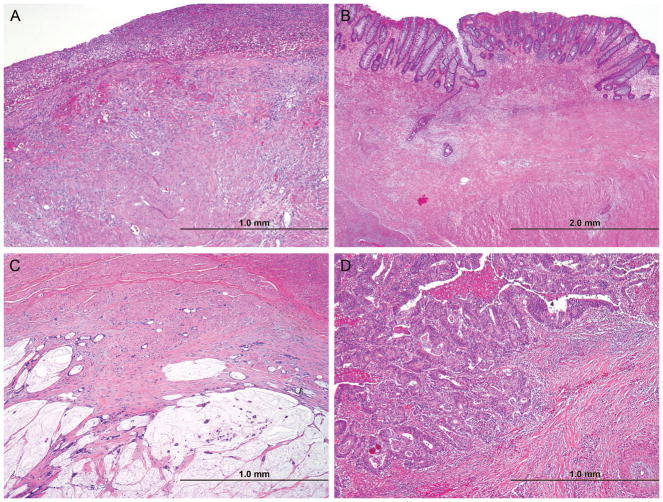
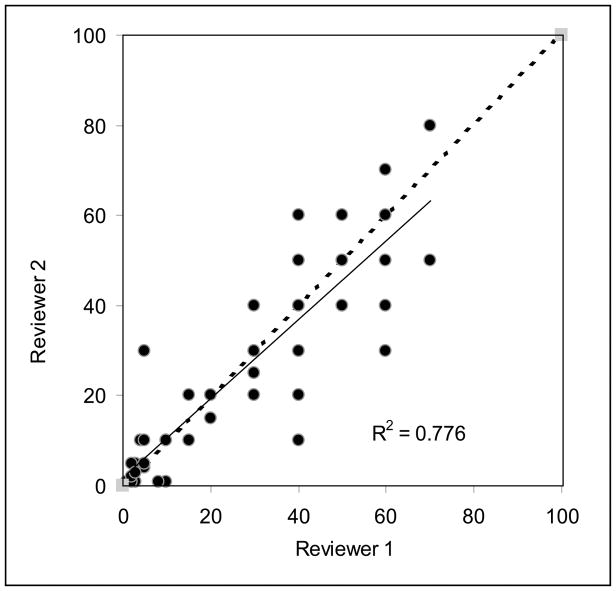
Methods: The authors studied 251 patients with rectal adenocarcinoma who were treated with neoadjuvant chemoradiation and radical resection. Quantified pathologic response was defined as an estimated percentage of residual cancer cells in relation to the tumor bed: complete, no residual cancer cells; near-complete, ≤ 5% residual cancer cells; major, > 5%, and < 50% residual cancer cells; and minor, ≥ 50% residual cancer cells. The reproducibility of quantified pathologic response between 2 pathologists was assessed using tumors from 55 randomly selected patients who did not demonstrate a complete response.
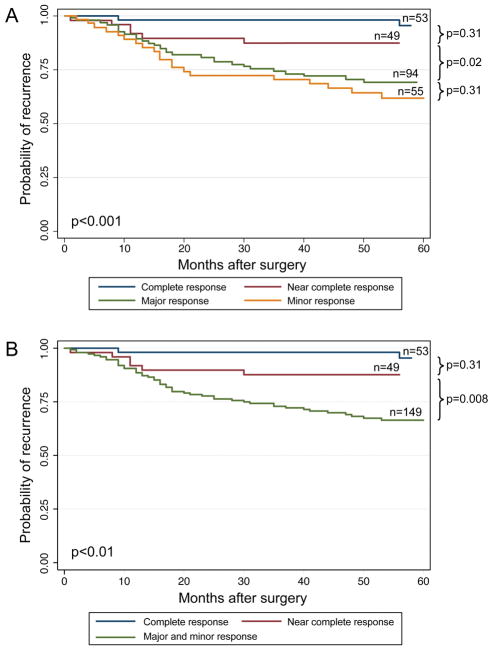
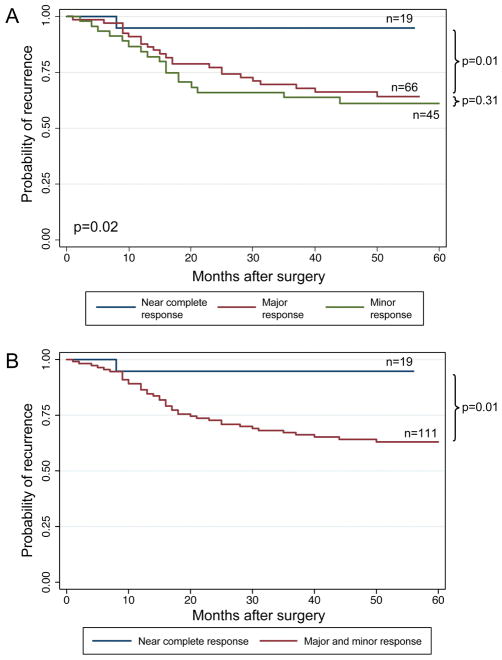
Results: Pathologic response was complete in 21% of patients, near-complete in 20% of patients, major in 37% of patients, and minor in 22% of patients. Nineteen percent of patients had ypT0N0 disease, 27% had ypT1-2N0 disease, 21% had ypT3-4N0 disease, and 33% had N+ disease. The 5-year RFS rates by category of quantified pathologic response were as follows: complete, 95%; near-complete, 88%; major, 69%; and minor, 61% (P < .001). Major and minor response, high histologic grade, and perineural invasion were found to be significant predictors of decreased RFS on multivariate analysis. The 5-year RFS rates for patients with ypT3-4 or N+ disease were better for those with a near-complete response (94%) compared with those with a major (64%) or minor (61%) response (P < .02). Moderate to substantial agreement was observed between the 2 pathologists (κ = 0.72).
Conclusions: Quantified pathologic response is a predictor of RFS in patients with rectal adenocarcinoma and stratifies patients with high pathologic stage disease.
Keywords: adenocarcinoma; cancer; chemoradiation; complete; near-complete; neoadjuvant therapy; pathologic response; preoperative; rectum; recurrence-free survival.
© 2013 American Cancer Society.
Figures
Comment in
-
Reply to Can quantified pathologic response assessed as residual tumor burden be a promising staging system for patients with rectal cancer treated with chemoradiation followed by surgery?Cancer. 2014 Apr 15;120(8):1282. doi: 10.1002/cncr.28559. Epub 2014 Jan 28. Cancer. 2014. PMID: 24474599 No abstract available.
-
Can quantified pathologic response assessed as residual tumor burden be a promising staging system for patients with rectal cancer treated with chemoradiation followed by surgery?Cancer. 2014 Apr 15;120(8):1281-2. doi: 10.1002/cncr.28560. Epub 2014 Jan 28. Cancer. 2014. PMID: 24474633 No abstract available.
References
-
- American Cancer Society. Cancer facts & figures 2012. Atlanta: American Cancer Society; 2012.
-
- Bosset J-F, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355:1114–1123. - PubMed
-
- Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638–646. - PubMed
-
- Maas M, Nelemans PJ, Valentini V, et al. Long term outcome in patients with pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol. 2010;11:835–844. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
