

Peripheral blood mononuclear cell gene expression profiles predict poor outcome in idiopathic pulmonary fibrosis
- PMID: 24089408
- PMCID: PMC4175518
- DOI: 10.1126/scitranslmed.3005964
Peripheral blood mononuclear cell gene expression profiles predict poor outcome in idiopathic pulmonary fibrosis
Abstract
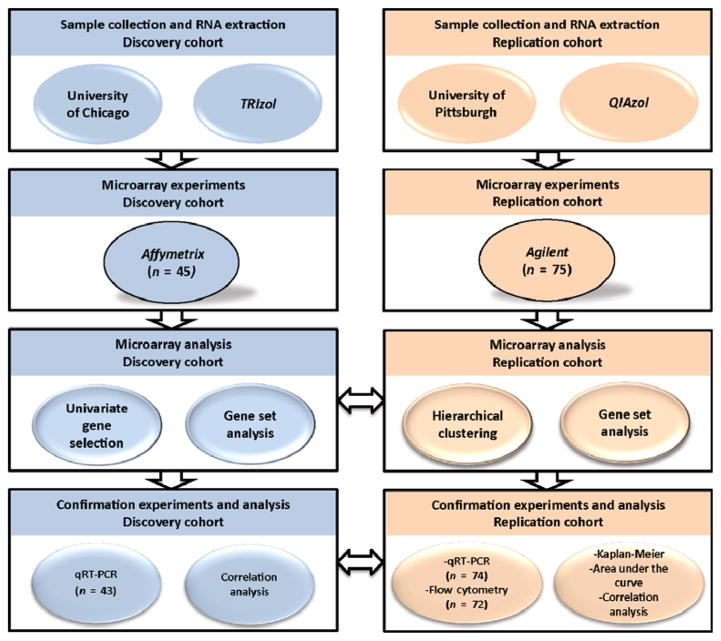
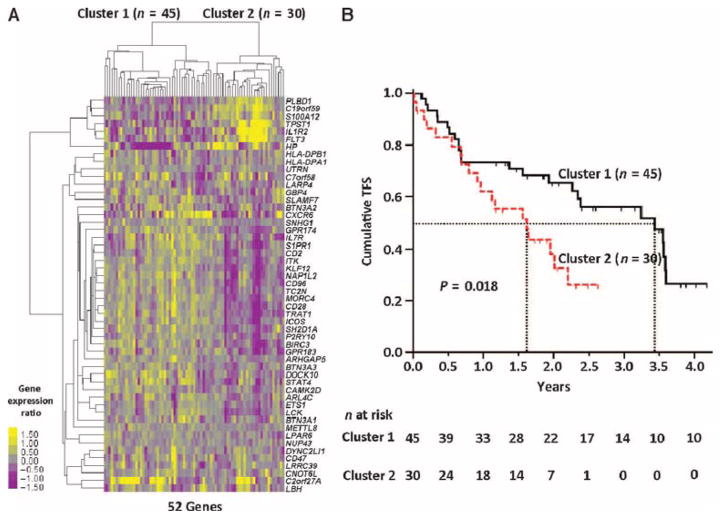
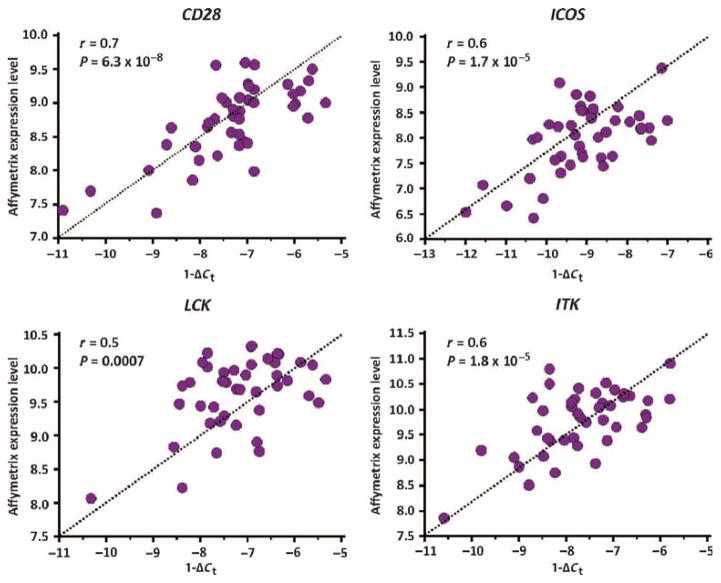
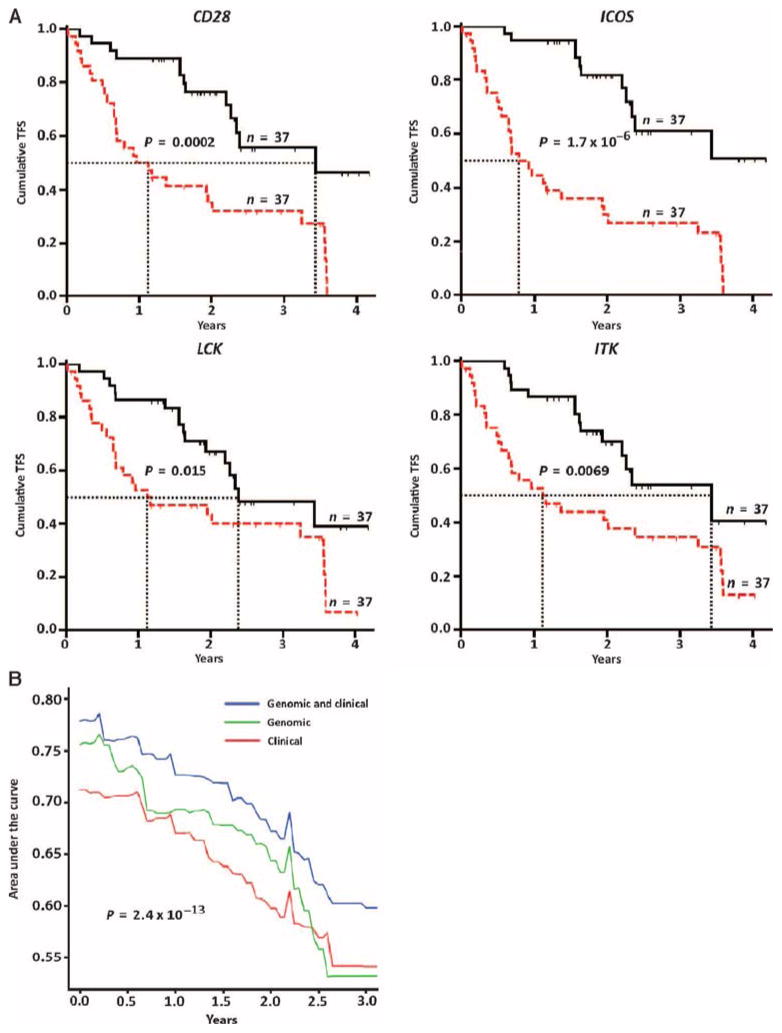
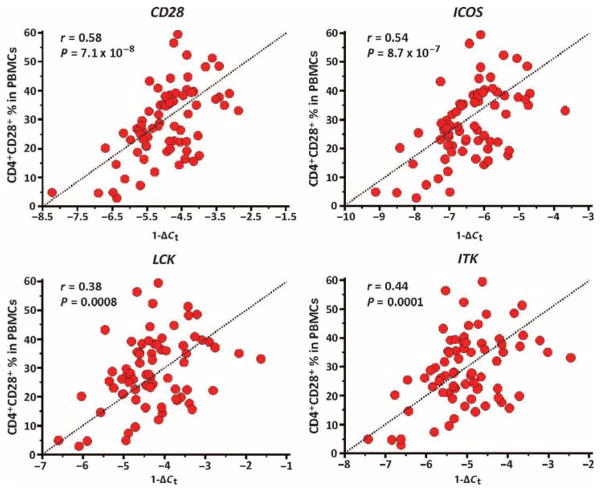
We aimed to identify peripheral blood mononuclear cell (PBMC) gene expression profiles predictive of poor outcomes in idiopathic pulmonary fibrosis (IPF) by performing microarray experiments of PBMCs in discovery and replication cohorts of IPF patients. Microarray analyses identified 52 genes associated with transplant-free survival (TFS) in the discovery cohort. Clustering the microarray samples of the replication cohort using the 52-gene outcome-predictive signature distinguished two patient groups with significant differences in TFS. We studied the pathways associated with TFS in each independent microarray cohort and identified decreased expression of "The costimulatory signal during T cell activation" Biocarta pathway and, in particular, the genes CD28, ICOS, LCK, and ITK, results confirmed by quantitative reverse transcription polymerase chain reaction (qRT-PCR). A proportional hazards model, including the qRT-PCR expression of CD28, ICOS, LCK, and ITK along with patient's age, gender, and percent predicted forced vital capacity (FVC%), demonstrated an area under the receiver operating characteristic curve of 78.5% at 2.4 months for death and lung transplant prediction in the replication cohort. To evaluate the potential cellular source of CD28, ICOS, LCK, and ITK expression, we analyzed and found significant correlation of these genes with the PBMC percentage of CD4(+)CD28(+) T cells in the replication cohort. Our results suggest that CD28, ICOS, LCK, and ITK are potential outcome biomarkers in IPF and should be further evaluated for patient prioritization for lung transplantation and stratification in drug studies.
Conflict of interest statement
Figures
References
-
- Schwartz DA, Helmers RA, Galvin JR, Van Fossen DS, Frees KL, Dayton CS, Burmeister LF, Hunninghake GW. Determinants of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1994;149:450–454. - PubMed
-
- King TE, Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: Scoring system and survival model. Am J Respir Crit Care Med. 2001;164:1171–1181. - PubMed
-
- Zappala CJ, Latsi PI, Nicholson AG, Colby TV, Cramer D, Renzoni EA, Hansell DM, du Bois RM, Wells AU. Marginal decline in forced vital capacity is associated with a poor outcome in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35:830–836. - PubMed
-
- Ley B, Ryerson CJ, Vittinghoff E, Ryu JH, Tomassetti S, Lee JS, Poletti V, Buccioli M, Elicker BM, Jones KD, King TE, Jr, Collard HR. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156:684–691. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL105371/HL/NHLBI NIH HHS/United States
- RC2 HL101740/HL/NHLBI NIH HHS/United States
- U10 HL080513/HL/NHLBI NIH HHS/United States
- P50 HL107172/HL/NHLBI NIH HHS/United States
- HL080513/HL/NHLBI NIH HHS/United States
- U01 HL108642/HL/NHLBI NIH HHS/United States
- R01 HL095397/HL/NHLBI NIH HHS/United States
- HL101740/HL/NHLBI NIH HHS/United States
- HL095397/HL/NHLBI NIH HHS/United States
- P50 HL084932/HL/NHLBI NIH HHS/United States
- R01 HL073241/HL/NHLBI NIH HHS/United States
- P01 HL098050/HL/NHLBI NIH HHS/United States
- HL98050/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- HL073241/HL/NHLBI NIH HHS/United States
- HL0894932/HL/NHLBI NIH HHS/United States
- HL108642/HL/NHLBI NIH HHS/United States
- HL107172/HL/NHLBI NIH HHS/United States
- HL105371/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
