

Infliximab dose reduction sustains the clinical treatment effect in active HLAB27 positive ankylosing spondylitis: a two-year pilot study
- PMID: 24089587
- PMCID: PMC3780705
- DOI: 10.1155/2013/289845
Infliximab dose reduction sustains the clinical treatment effect in active HLAB27 positive ankylosing spondylitis: a two-year pilot study
Abstract
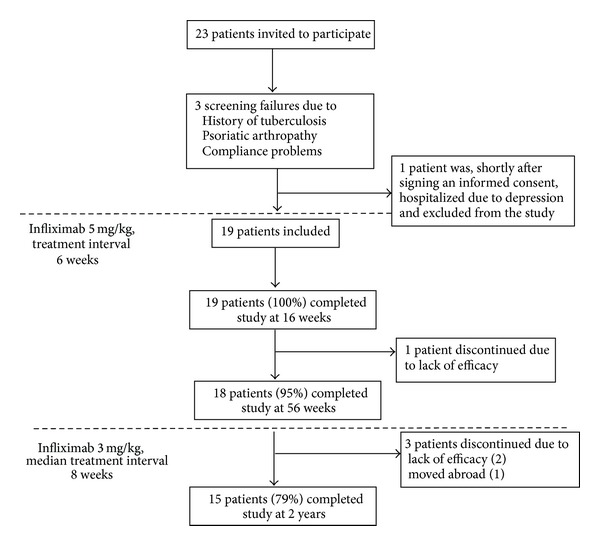
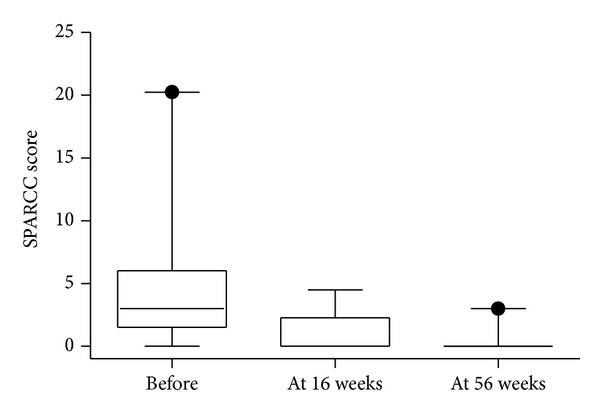
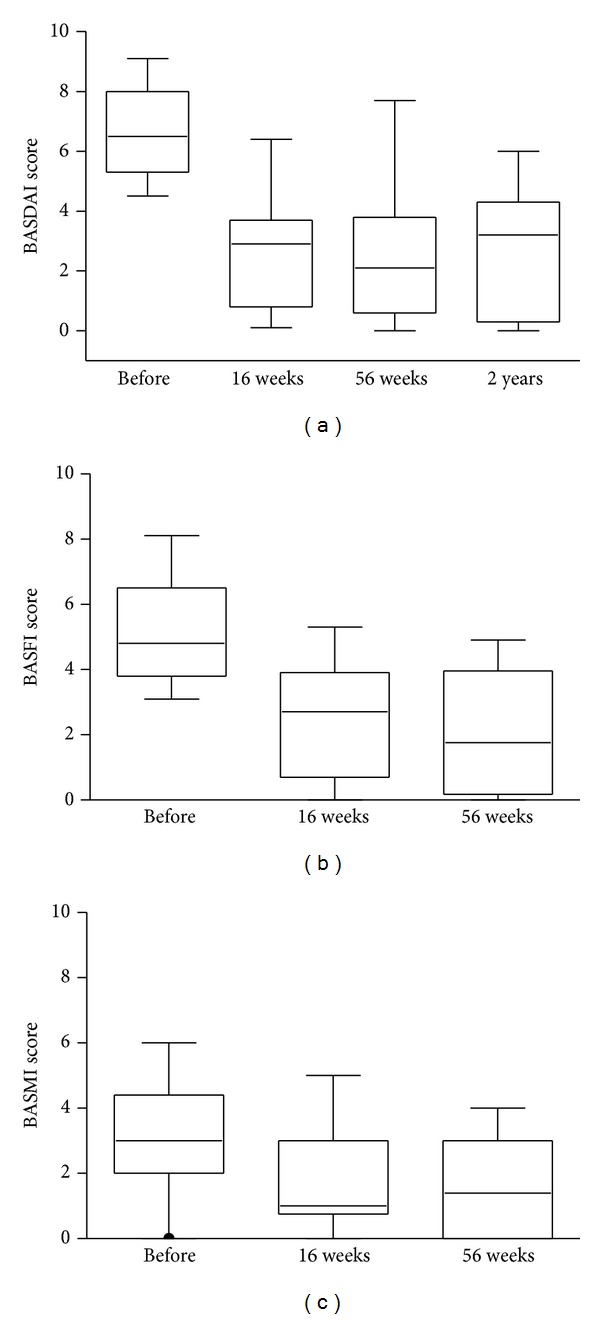
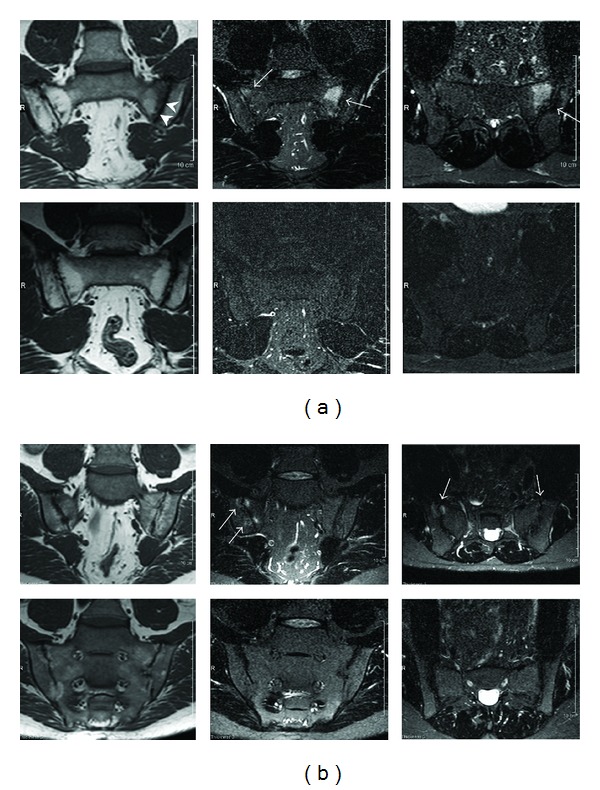
The rationale of the study was to evaluate the efficacy of infliximab (IFX) treatment in patients with ankylosing spondylitis (AS) and to determine whether IFX dose reduction and interval extension sustains the treatment effect. Nineteen patients were included and treated with IFX 5 mg/kg every 6 weeks for 56 weeks. All patients concomitantly received MTX with median dose 7.5 mg/weekly. During the second year, the IFX dose was reduced to 3 mg/kg every 8 weeks. Eighteen patients completed the 1-year and 15 patients the 2-year trial. The ≥50% improvement at week 16 from baseline of BASDAI was achieved in 16/19 (84%) patients. Significant reductions in BASDAI, BASFI, and BASMI scores, decrease in ESR and CRP, and improvement in SF-36 were observed at weeks 16 and 56. The MRI-defined inflammatory changes in the sacroiliac joints disappeared in 10/15 patients (67%) already at 16 weeks. IFX treatment effect was sustained throughout the second year after IFX dose reduction and interval extension. We conclude that IFX treatment is effective in well-established active AS and a dose reduction sustains the treatment effect. These observations are of clinical importance and open the opportunity to reduce the drug costs.
Trial registration: ClinicalTrials.gov NCT01850121.
Figures

Similar articles
-
Increased efficacy of infliximab associated with methotrexate in ankylosing spondylitis.Joint Bone Spine. 2007 May;74(3):254-8. doi: 10.1016/j.jbspin.2006.08.005. Epub 2007 Mar 1. Joint Bone Spine. 2007. PMID: 17387031 Clinical Trial.
-
Clinical and imaging efficacy of infliximab in HLA-B27-Positive patients with magnetic resonance imaging-determined early sacroiliitis.Arthritis Rheum. 2009 Apr;60(4):946-54. doi: 10.1002/art.24408. Arthritis Rheum. 2009. PMID: 19333933 Clinical Trial.
-
Infliximab in ankylosing spondylitis: a prospective observational inception cohort analysis of efficacy and safety.J Rheumatol. 2002 May;29(5):959-65. J Rheumatol. 2002. PMID: 12022358 Clinical Trial.
-
Propensity score matching/reweighting analysis comparing intravenous golimumab to infliximab for ankylosing spondylitis using data from the GO-ALIVE and ASSERT trials.Clin Rheumatol. 2020 Oct;39(10):2907-2917. doi: 10.1007/s10067-020-05051-1. Epub 2020 May 4. Clin Rheumatol. 2020. PMID: 32367407 Free PMC article.
-
A double-blind, placebo-controlled trial of low dose infliximab in ankylosing spondylitis.J Rheumatol. 2010 Jun;37(6):1203-10. doi: 10.3899/jrheum.091042. Epub 2010 Mar 15. J Rheumatol. 2010. PMID: 20231198 Clinical Trial.
Cited by
-
Practical recommendations for the use of therapeutic drug monitoring of biopharmaceuticals in inflammatory diseases.Clin Pharmacol. 2017 Oct 3;9:101-111. doi: 10.2147/CPAA.S138414. eCollection 2017. Clin Pharmacol. 2017. PMID: 29042821 Free PMC article. Review.
-
Dose Tapering and Discontinuation of Biologic DMARDs in Axial Spondyloarthritis: A Narrative Review (2023 SPARTAN Annual Meeting Proceedings).Curr Rheumatol Rep. 2024 May;26(5):155-163. doi: 10.1007/s11926-024-01137-w. Epub 2024 Feb 9. Curr Rheumatol Rep. 2024. PMID: 38332457 Free PMC article. Review.
-
Factors related to health-related quality of life in ankylosing spondylitis, overall and stratified by sex.Arthritis Res Ther. 2018 Dec 27;20(1):284. doi: 10.1186/s13075-018-1784-8. Arthritis Res Ther. 2018. PMID: 30587228 Free PMC article. Clinical Trial.
-
Response to lower dose TNF inhibitors in axial spondyloarthritis; a real-world multicentre observational study.Rheumatol Adv Pract. 2020 May 13;4(2):rkaa015. doi: 10.1093/rap/rkaa015. eCollection 2020. Rheumatol Adv Pract. 2020. PMID: 32793854 Free PMC article.
-
Pan American League of Associations for Rheumatology recommendations for the management of axial spondyloarthritis.Nat Rev Rheumatol. 2023 Nov;19(11):724-737. doi: 10.1038/s41584-023-01034-z. Epub 2023 Oct 6. Nat Rev Rheumatol. 2023. PMID: 37803079
References
-
- Brandt J, Bollow M, Häberle J, et al. Studying patients with inflammatory back pain and arthritis of the lower limbs clinically and by magnetic resonance imaging: many, but not all patients with sacroiliitis have spondyloarthropathy. Rheumatology. 1999;38(9):831–836. - PubMed
-
- Braun J, Bollow M, Remlinger G, et al. Prevalence of spondylarthropathies in HLA-B27 positive and negative blood donors. Arthritis and Rheumatism. 1998;41(1):58–67. - PubMed
-
- Boonen A. A review of work-participation, cost-of-illness and cost-effectiveness studies in ankylosing spondylitis. Nature Clinical Practice Rheumatology. 2006;2(10):546–553. - PubMed
-
- van der Heijde D, Dijkmans B, Geusens P, et al. Efficacy and safety of infliximab in patients with ankylosing spondylitis: results of a randomized, placebo-controlled trial (ASSERT) Arthritis and Rheumatism. 2005;52(2):582–591. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
