

Spontaneous lateral sphenoid cephaloceles: anatomic factors contributing to pathogenesis and proposed classification
- PMID: 24091443
- PMCID: PMC7965830
- DOI: 10.3174/ajnr.A3744
Spontaneous lateral sphenoid cephaloceles: anatomic factors contributing to pathogenesis and proposed classification
Abstract
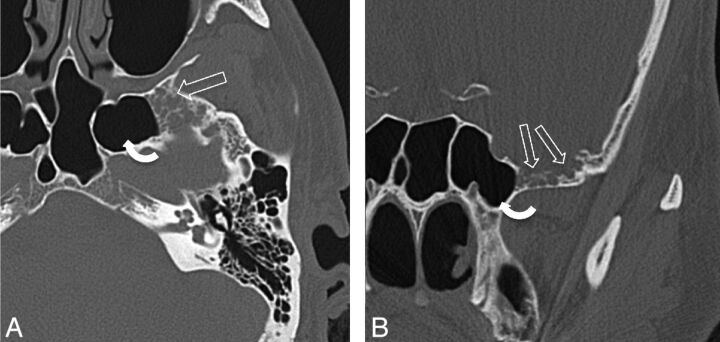
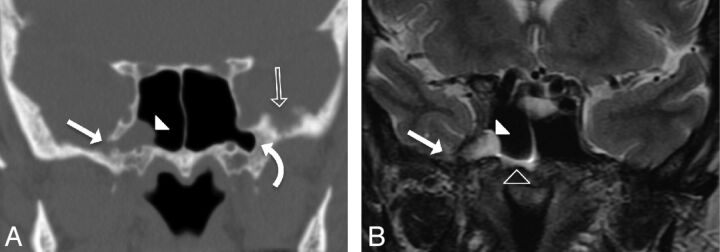
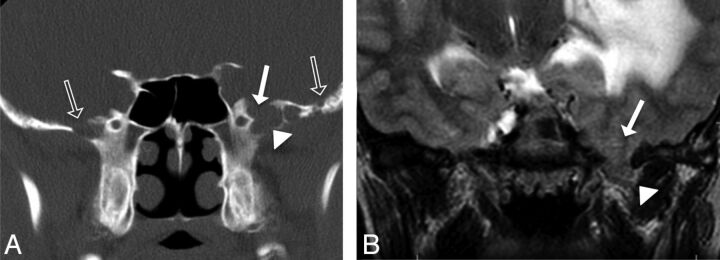
Spontaneous lateral sphenoid cephaloceles arise from bony defects in the lateral sphenoid, in the absence of predisposing factors such as trauma, surgery, mass, or congenital skull base malformation. We reviewed CT and MR imaging findings and clinical data of 26 patients with spontaneous lateral sphenoid cephaloceles to better understand anatomic contributions to pathogenesis, varying clinical and imaging manifestations, and descriptive terminology. Two types of spontaneous lateral sphenoid cephaloceles were identified. In 15 of 26 patients, a type 1 spontaneous lateral sphenoid cephalocele was noted, herniating into a pneumatized lateral recess of the sphenoid sinus, and typically presenting with CSF leak and/or headache. In 11 of 26 patients, a type 2 spontaneous lateral sphenoid cephalocele was noted, isolated to the greater sphenoid wing without extension into the sphenoid sinus, presenting with seizures, headaches, meningitis, cranial neuropathy, or detected incidentally. All patients had sphenoid arachnoid pits, and 61% of patients had an empty or partially empty sella, suggesting that altered CSF dynamics may play a role in their genesis.
Figures
References
-
- Lloyd KM, DelGaudio JM, Hudgins PA. Imaging of skull base cerebrospinal fluid leaks in adults. Radiology 2008;248:725–36 - PubMed
-
- Lopatin AS, Kapitanov DN, Potapov AA. Endonasal endoscopic repair of spontaneous cerebrospinal fluid leaks. Arch Otolaryngol Head Neck Surg 2003;129:859–63 - PubMed
-
- Alonso RC, de la Peña MJ, Caicoya AG, et al. Spontaneous skull base meningoencephaloceles and cerebrospinal fluid fistulas. Radiographics 2013;33:553–70 - PubMed
-
- Meco C, Oberascher G. Comprehensive algorithm for skull base dural lesion and cerebrospinal fluid fistula diagnosis. Laryngoscope 2004;114:991–99 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources