

A validated risk model to predict 90-day VTE events in postsurgical patients
- PMID: 24091567
- PMCID: PMC4502716
- DOI: 10.1378/chest.13-1553
A validated risk model to predict 90-day VTE events in postsurgical patients
Abstract
Background: VTE is the proximate cause of 100,000 deaths in the United States each year. Perioperative VTE risk among surgical patients varies by 20-fold, which highlights the importance of risk stratification to identify high-risk patients, in whom chemoprophylaxis can decrease VTE risk, and low-risk patients, for whom the risk-benefit relationship of prophylaxis may be unfavorable.
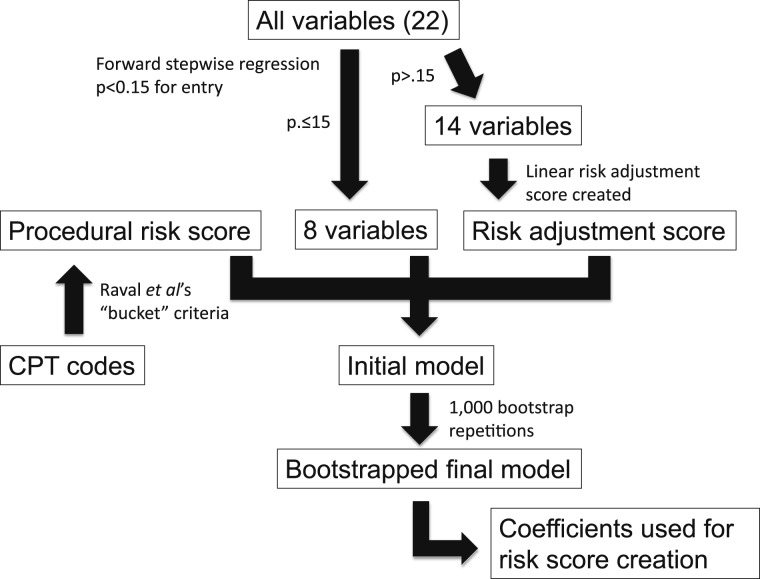
Methods: We used data from a statewide surgical quality collaborative for surgical procedures performed between 2010 and 2012. Regression-based techniques identified predictors of 90-day VTE while adjusting for procedural complexity and comorbid conditions. A weighted risk index was created and was validated subsequently in a separate, independent dataset.
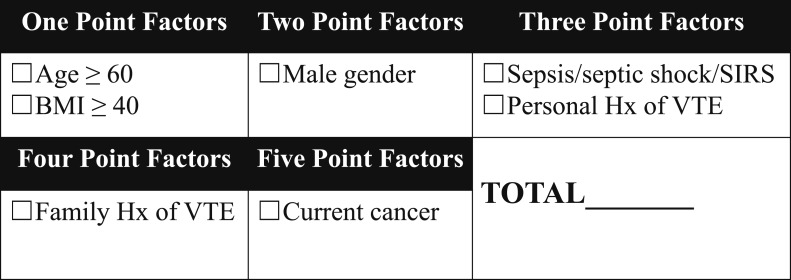
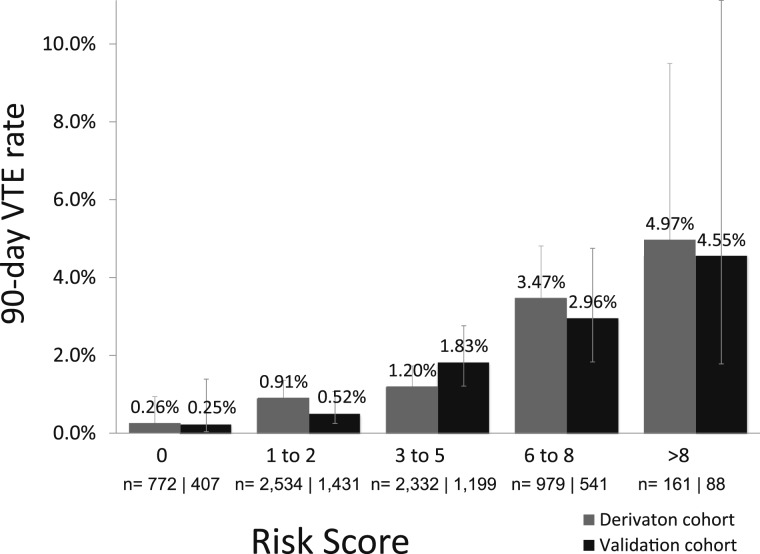
Results: Data were available for 10,344 patients, who were allocated randomly to a derivation or validation cohort. The 90-day VTE rate was 1.4%; 66.2% of the derivation cohort and 65.5% of the validation cohort received chemoprophylaxis. Seven risk factors were incorporated into a weighted risk index: personal history of VTE, current cancer, sepsis/septic shock/systemic inflammatory response syndrome, age≥60 years, BMI≥40 kg/m2, male sex, and family history of VTE. Prediction for 90-day VTE was similar in the derivation and validation cohorts (areas under the receiver operator curve, 0.72 and 0.70, respectively). An 18-fold variation in 90-day VTE rate was identified.
Conclusions: A weighted risk index quantifies 90-day VTE risk among surgical patients and identifies an 18-fold variation in VTE risk among the overall surgical population.
Figures
Similar articles
-
Inadequate venous thromboembolism risk stratification predicts venous thromboembolic events in surgical intensive care unit patients.J Am Coll Surg. 2014 May;218(5):898-904. doi: 10.1016/j.jamcollsurg.2014.01.046. Epub 2014 Feb 25. J Am Coll Surg. 2014. PMID: 24680577
-
Risk factors and pharmacologic prophylaxis for venous thromboembolism in elective spine surgery.Spine J. 2018 Jun;18(6):970-978. doi: 10.1016/j.spinee.2017.10.013. Epub 2017 Oct 19. Spine J. 2018. PMID: 29056565
-
Association of Perioperative Red Blood Cell Transfusions With Venous Thromboembolism in a North American Registry.JAMA Surg. 2018 Sep 1;153(9):826-833. doi: 10.1001/jamasurg.2018.1565. JAMA Surg. 2018. PMID: 29898202 Free PMC article.
-
The use of weighted and scored risk assessment models for venous thromboembolism.Thromb Haemost. 2012 Dec;108(6):1072-6. doi: 10.1160/TH12-07-0508. Epub 2012 Nov 8. Thromb Haemost. 2012. PMID: 23138506 Review.
-
Asian venous thromboembolism guidelines: prevention of venous thromboembolism.Int Angiol. 2012 Dec;31(6):501-16. Int Angiol. 2012. PMID: 23222928 Review.
Cited by
-
A retrospective analysis based on multiple machine learning models to predict lymph node metastasis in early gastric cancer.Front Oncol. 2022 Dec 1;12:1023110. doi: 10.3389/fonc.2022.1023110. eCollection 2022. Front Oncol. 2022. PMID: 36530978 Free PMC article.
-
Untapped potential of multicenter studies: a review of cardiovascular risk prediction models revealed inappropriate analyses and wide variation in reporting.Diagn Progn Res. 2019 Feb 22;3:6. doi: 10.1186/s41512-019-0046-9. eCollection 2019. Diagn Progn Res. 2019. PMID: 31093576 Free PMC article. Review.
-
Venous thromboembolism (VTE) prophylaxis after bariatric surgery: a national survey of MBSAQIP director practices.Surg Obes Relat Dis. 2023 Aug;19(8):799-807. doi: 10.1016/j.soard.2022.12.038. Epub 2023 Jan 2. Surg Obes Relat Dis. 2023. PMID: 36717309 Free PMC article.
-
Incidence of Venous Thromboembolism Following Major Emergency Abdominal Surgery.World J Surg. 2020 Mar;44(3):704-710. doi: 10.1007/s00268-019-05246-x. World J Surg. 2020. PMID: 31646367
-
Risk assessment models for venous thromboembolism in hospitalised adult patients: a systematic review.BMJ Open. 2021 Jul 29;11(7):e045672. doi: 10.1136/bmjopen-2020-045672. BMJ Open. 2021. PMID: 34326045 Free PMC article.
References
-
- Anderson FA, Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82(9):777-782. - PubMed
-
- Goldhaber SZ. Venous thromboembolism risk among hospitalized patients: magnitude of the risk is staggering. Am J Hematol. 2007;82(9):775-776. - PubMed
-
- Centers for Disease Control and Prevention (CDC). Venous thromboembolism in adult hospitalizations - United States, 2007-2009. MMWR Morb Mortal Wkly Rep. 2012;61(22):401-404. - PubMed
-
- Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21(1):23-29. - PubMed
-
- The Surgeon General’s call to action to prevent deep vein thrombosis and pulmonary embolism. Surgeon General website. http://www.surgeongeneral.gov/library/calls/index.html. Accessed February 12, 2013. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
