

Cancer-initiating cells derived from human rectal adenocarcinoma tissues carry mesenchymal phenotypes and resist drug therapies
- PMID: 24091671
- PMCID: PMC3824647
- DOI: 10.1038/cddis.2013.337
Cancer-initiating cells derived from human rectal adenocarcinoma tissues carry mesenchymal phenotypes and resist drug therapies
Abstract
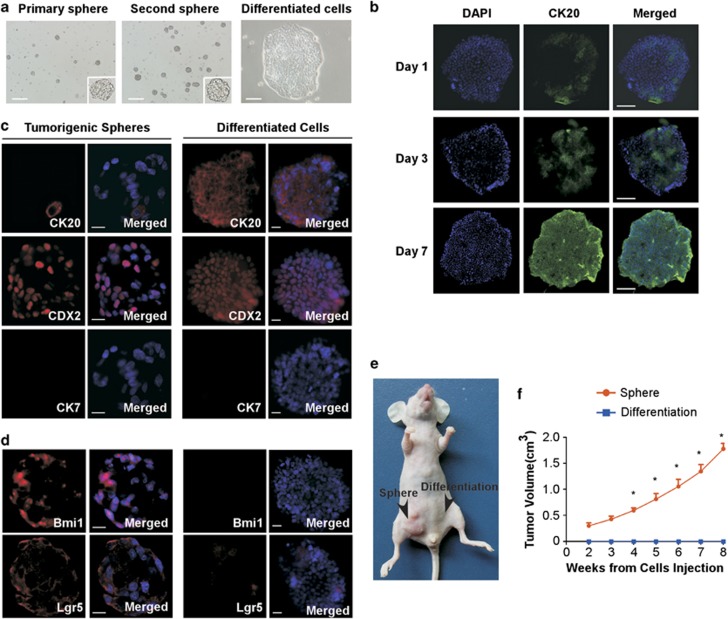
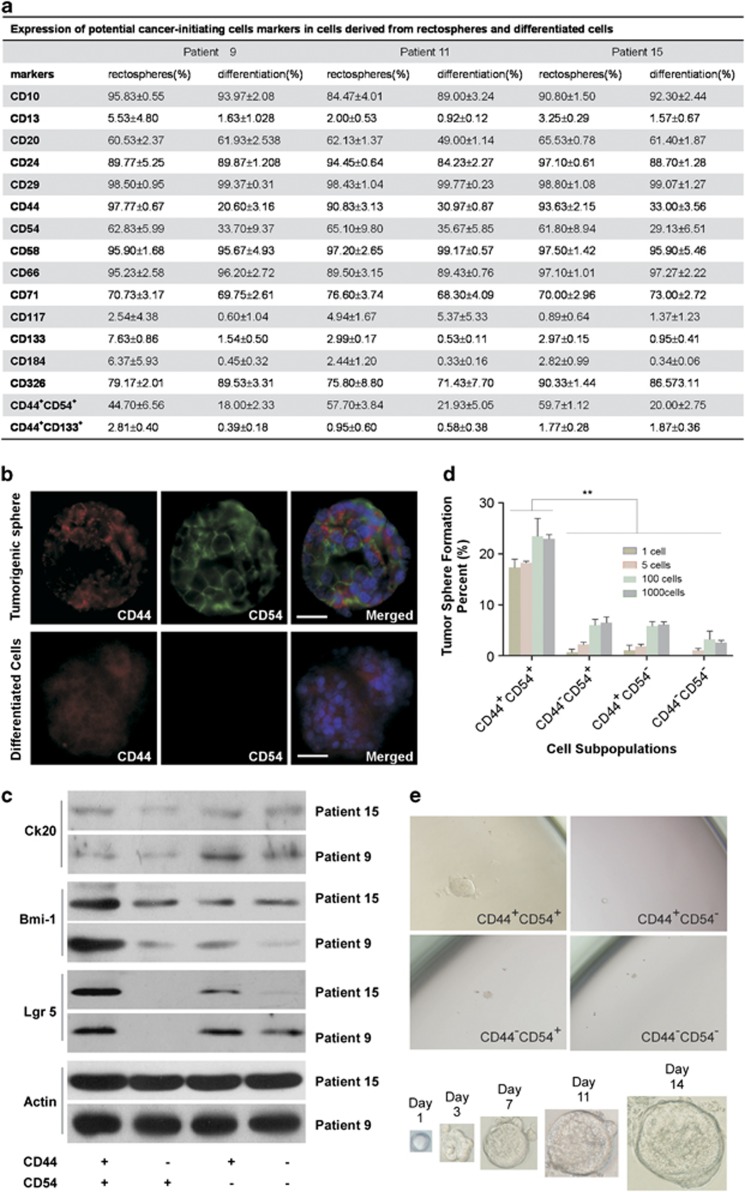
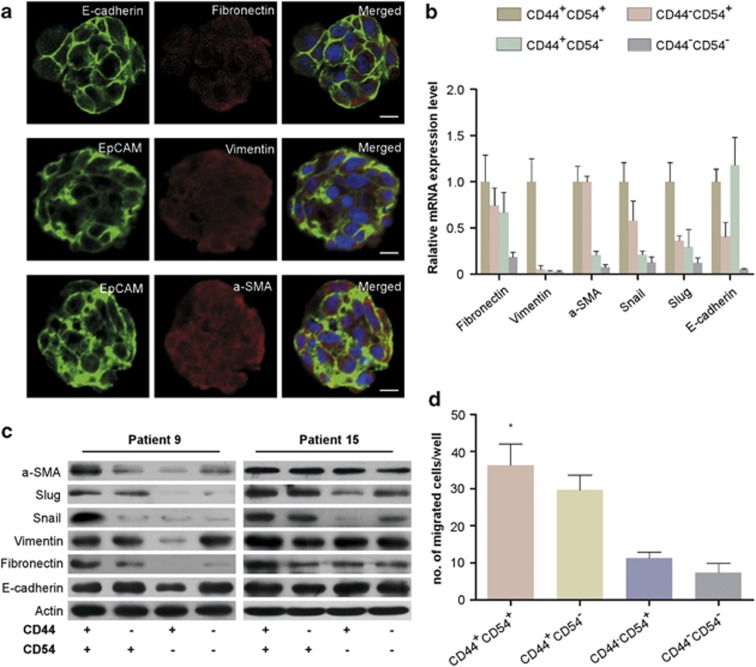
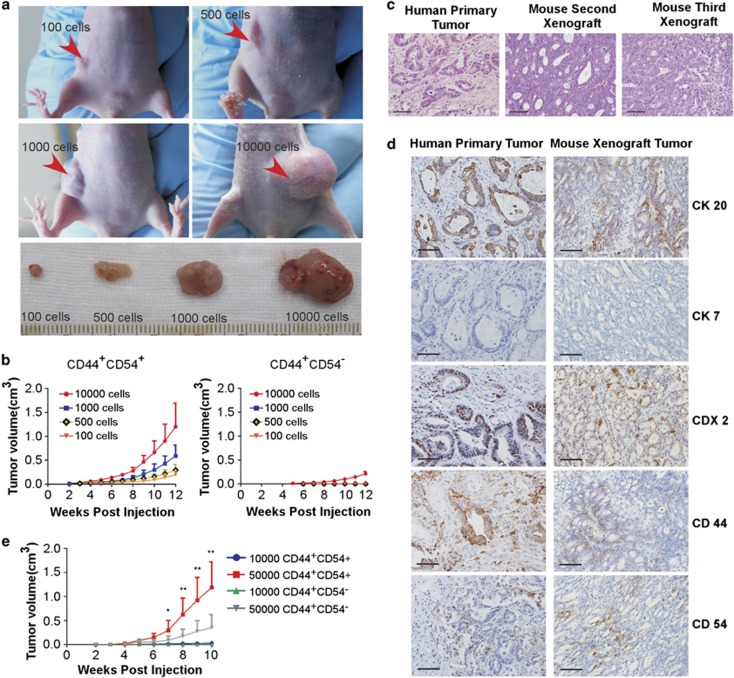
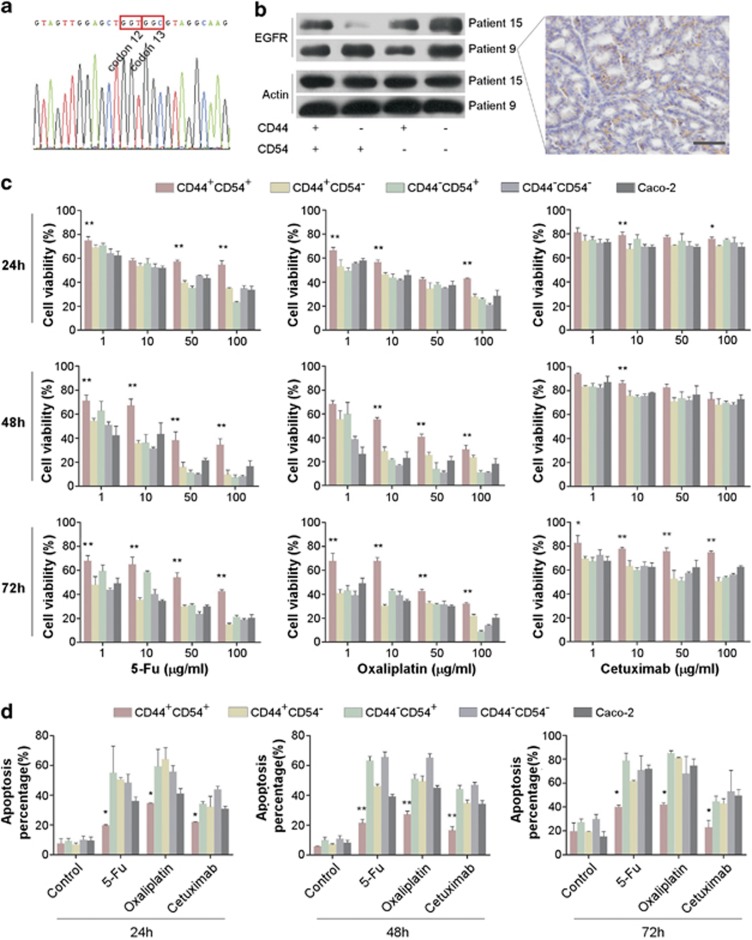
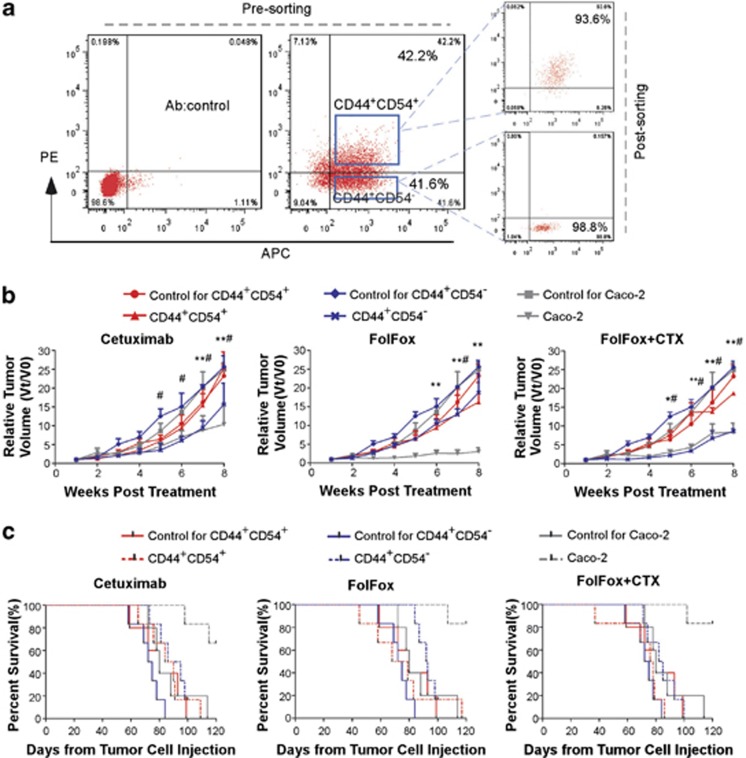
Accumulating evidence indicates that cancer-initiating cells (CICs) are responsible for cancer initiation, relapse, and metastasis. Colorectal carcinoma (CRC) is typically classified into proximal colon, distal colon, and rectal cancer. The gradual changes in CRC molecular features within the bowel may have considerable implications in colon and rectal CICs. Unfortunately, limited information is available on CICs derived from rectal cancer, although colon CICs have been described. Here we identified rectal CICs (R-CICs) that possess differentiation potential in tumors derived from patients with rectal adenocarcinoma. The R-CICs carried both CD44 and CD54 surface markers, while R-CICs and their immediate progenies carried potential epithelial-mesenchymal transition characteristics. These R-CICs generated tumors similar to their tumor of origin when injected into immunodeficient mice, differentiated into rectal epithelial cells in vitro, and were capable of self-renewal both in vitro and in vivo. More importantly, subpopulations of R-CICs resisted both 5-fluorouracil/calcium folinate/oxaliplatin (FolFox) and cetuximab treatment, which are the most common therapeutic regimens used for patients with advanced or metastatic rectal cancer. Thus, the identification, expansion, and properties of R-CICs provide an ideal cellular model to further investigate tumor progression and determine therapeutic resistance in these patients.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics. CA Cancer J Clin. 2010;2010;60:277–300. - PubMed
-
- Yu H, Harris RE, Gao YT, Gao R, Wynder EL. Comparative epidemiology of cancers of the colon, rectum, prostate and breast in Shanghai, China versus the United States. Int J Epidemiol. 1991;20:76–81. - PubMed
-
- Cunningham D, Atkin W, Lenz HJ, Lynch HT, Minsky B, Nordlinger B, et al. Colorectal cancer. Lancet. 2010;375:1030–1047. - PubMed
-
- Ricci-Vitiani L, Fabrizi E, Palio E, De Maria R. Colon cancer stem cells. J Mol Med. 2009;87:1097–1104. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
