

Posterior fixation of thoracolumbar burst fractures: is it possible to protect one segment in the lumbar region?
- PMID: 24091822
- PMCID: PMC3990854
- DOI: 10.1007/s00590-013-1326-7
Posterior fixation of thoracolumbar burst fractures: is it possible to protect one segment in the lumbar region?
Abstract
Background: The treatment for thoracolumbar burst fractures is controversial. The aim of this retrospective study was to compare intermediate-segment (IS) and long-segment (LS) instrumentation in the treatment for these fractures.
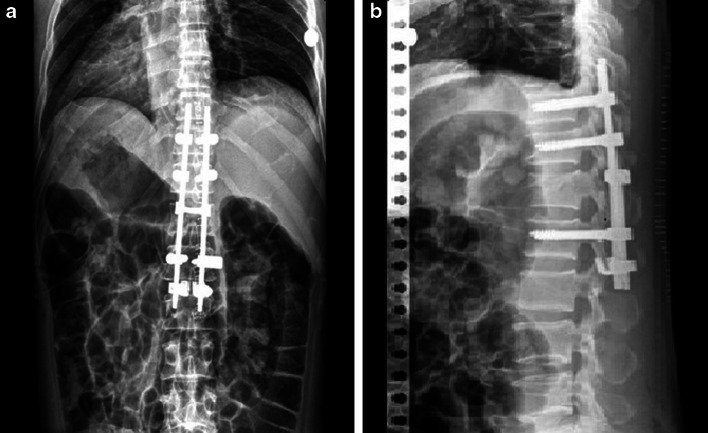
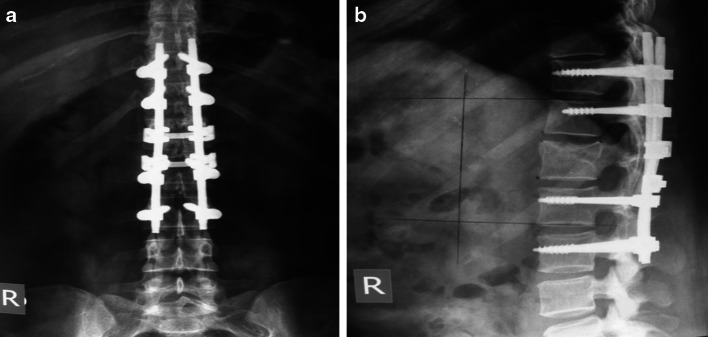
Methods: IS instrumentation was considered as pedicle fixation two levels above and one level below the fractured vertebra (infra-laminar hooks attached to lower vertebra with pedicle screws). LS instrumentation was done two levels above and two levels below the fractured vertebra. Among a total of 25 consecutive patients, Group 1 included ten patients treated by IS pedicle fixation, whereas Group 2 included fifteen patients treated by LS instrumentation.
Results: The measurements of local kyphosis (p = 0.955), sagittal index (p = 0.128), anterior vertebral height compression (p = 0.230) and canal diameter expansion (p = 0.839) demonstrated similar improvement at the final follow-up between the two groups. However, there was a significant difference (p < 0.05) between Group 1 and Group 2 regarding clinical outcome [Hannover scoring system, Oswestry disability questionnaire and the range of motion of the lumbar region compared to neutral (0°)].
Conclusions: The radiographic parameters were the same between the two groups. However, the clinical parameters demonstrated that IS instrumentation is a more effective management of thoracolumbar burst fractures.
Figures

References
-
- Mumford J, Weinstein JN, Spratt KF, Goel VK (1993) Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976) 18(8):955–970 - PubMed
-
- Hitchon PW, Torner JC, Haddad SF, Follett KA (1998) Management options in thoracolumbar burst fractures. Surg Neurol 49(6):619–626; 626–627 - PubMed
-
- Chen HH, Wang WK, Li KC, Chen TH (2004) Biomechanical effects of the body augmenter for reconstruction of the vertebral body. Spine (Phila Pa 1976) 29(18):E382–E387 - PubMed
-
- Parker JW, Lane JR, Karaikovic EE, Gaines RW (2000) Successful short-segment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 41/2-year series. Spine (Phila Pa 1976) 25(9):1157–1170 - PubMed
-
- Kaneda K, Taneichi H, Abumi K, Hashimoto T, Satoh S, Fujiya M. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Joint Surg [Am] 1997;79(1):69–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
