

Clinical utility of viral load in management of cytomegalovirus infection after solid organ transplantation
- PMID: 24092851
- PMCID: PMC3811235
- DOI: 10.1128/CMR.00015-13
Clinical utility of viral load in management of cytomegalovirus infection after solid organ transplantation
Abstract
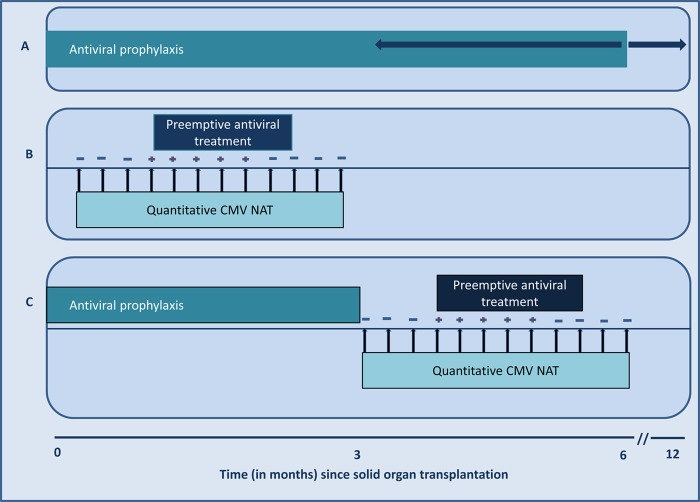
The negative impact of cytomegalovirus (CMV) infection on transplant outcomes warrants efforts toward improving its prevention, diagnosis, and treatment. During the last 2 decades, significant breakthroughs in diagnostic virology have facilitated remarkable improvements in CMV disease management. During this period, CMV nucleic acid amplification testing (NAT) evolved to become one of the most commonly performed tests in clinical virology laboratories. NAT provides a means for rapid and sensitive diagnosis of CMV infection in transplant recipients. Viral quantification also introduced several principles of CMV disease management. Specifically, viral load has been utilized (i) for prognostication of CMV disease, (ii) to guide preemptive therapy, (iii) to assess the efficacy of antiviral treatment, (iv) to guide the duration of treatment, and (v) to indicate the risk of clinical relapse or antiviral drug resistance. However, there remain important limitations that require further optimization, including the interassay variability in viral load reporting, which has limited the generation of standardized viral load thresholds for various clinical indications. The recent introduction of an international reference standard should advance the major goal of uniform viral load reporting and interpretation. However, it has also become apparent that other aspects of NAT should be standardized, including sample selection, nucleic acid extraction, amplification, detection, and calibration, among others. This review article synthesizes the vast amount of information on CMV NAT and provides a timely review of the clinical utility of viral load testing in the management of CMV in solid organ transplant recipients. Current limitations are highlighted, and avenues for further research are suggested to optimize the clinical application of NAT in the management of CMV after transplantation.
Figures


References
-
- Beam E, Razonable RR. 2012. Cytomegalovirus in solid organ transplantation: epidemiology, prevention, and treatment. Curr. Infect. Dis. Rep. 14:633–641 - PubMed
-
- Razonable R, Humar A. 2013. Cytomegalovirus in solid organ transplant recipients. Am. J. Transplant. 13:93–106 - PubMed
-
- Razonable R, Asberg A, Rollag H, Duncan J, Boisvert D, Yao JD, Caliendo AM, Humar A, Do T. 2013. Viral load suppression as measured by a CMV test calibrated to the WHO international standard is predictive of CMV disease resolution in transplant recipients. Clin. Infect. Dis. 56:1546–1553 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
