

Blood pressure lowering and major cardiovascular events in people with and without chronic kidney disease: meta-analysis of randomised controlled trials
- PMID: 24092942
- PMCID: PMC3789583
- DOI: 10.1136/bmj.f5680
Blood pressure lowering and major cardiovascular events in people with and without chronic kidney disease: meta-analysis of randomised controlled trials
Abstract
Objective: To define the cardiovascular effects of lowering blood pressure in people with chronic kidney disease.
Design: Collaborative prospective meta-analysis of randomised trials.
Data sources and eligibility: Participating randomised trials of drugs to lower blood pressure compared with placebo or each other or that compare different blood pressure targets, with at least 1000 patient years of follow-up per arm.
Main outcome measures: Major cardiovascular events (stroke, myocardial infarction, heart failure, or cardiovascular death) in composite and individually and all cause death.
Participants: 26 trials (152,290 participants), including 30,295 individuals with reduced estimated glomerular filtration rate (eGFR), which was defined as eGFR <60 mL/min/1.73 m(2).
Data extraction: Individual participant data were available for 23 trials, with summary data from another three. Meta-analysis according to baseline kidney function was performed. Pooled hazard ratios per 5 mm Hg lower blood pressure were estimated with a random effects model.
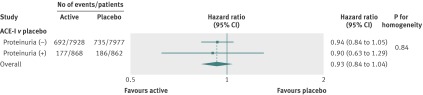
Results: Compared with placebo, blood pressure lowering regimens reduced the risk of major cardiovascular events by about a sixth per 5 mm Hg reduction in systolic blood pressure in individuals with (hazard ratio 0.83, 95% confidence interval 0.76 to 0.90) and without reduced eGFR (0.83, 0.79 to 0.88), with no evidence for any difference in effect (P=1.00 for homogeneity). The results were similar irrespective of whether blood pressure was reduced by regimens based on angiotensin converting enzyme inhibitors, calcium antagonists, or diuretics/β blockers. There was no evidence that the effects of different drug classes on major cardiovascular events varied between patients with different eGFR (all P>0.60 for homogeneity).
Conclusions: Blood pressure lowering is an effective strategy for preventing cardiovascular events among people with moderately reduced eGFR. There is little evidence from these overviews to support the preferential choice of particular drug classes for the prevention of cardiovascular events in chronic kidney disease.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures






Comment in
-
Do black patients with chronic kidney disease benefit equally from all blood pressure lowering agents?BMJ. 2014 Jan 15;348:g142. doi: 10.1136/bmj.g142. BMJ. 2014. PMID: 24429920 Free PMC article. No abstract available.
-
Authors' reply to Ladapo and Ogedegbe.BMJ. 2014 Jan 15;348:g148. doi: 10.1136/bmj.g148. BMJ. 2014. PMID: 24429921 No abstract available.
References
-
- Perkovic V, Cass A, Patel A, Suriyawongpaisal P, Barzi F, Chadban S, et al; InterASIA Collaborative Group. High prevalence of chronic kidney disease in Thailand. Kidney Int 2008;73:473-9. - PubMed
-
- Chadban SJ, Briganti EM, Kerr PG, Dunstan DW, Welborn TA, Zimmet PZ, et al. Prevalence of kidney damage in Australian adults: the AusDiab kidney study. J Am Soc Nephrol 2003;14(7 suppl 2):S131-8. - PubMed
-
- Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 2003;41:1-12. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al; American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003;108:2154-69. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004;351:1296-305. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous